Neuro-Ophthalmology
10.1 Anisocoria
Eyelid position, globe position (e.g., to rule out proptosis) and extraocular motility MUST be evaluated when anisocoria is present (see Figure 10.1.1).
Classification
The abnormal pupil is constricted.
Unilateral exposure to a miotic agent (e.g., pilocarpine).
Iritis: Eye pain, redness, and anterior chamber cell and flare.
 NOTE: In cases of inflammation resulting in posterior synechiae formation, the abnormal pupil may appear irregular, nonreactive, and/or larger.
NOTE: In cases of inflammation resulting in posterior synechiae formation, the abnormal pupil may appear irregular, nonreactive, and/or larger.
Horner syndrome: Mild ptosis on the side of the small pupil. SEE 10.2, HORNER SYNDROME.
Argyll Robertson (i.e., syphilitic) pupil: Always bilateral, irregularly round miotic pupils, but a mild degree of anisocoria is often present. SEE 10.3, ARGYLL ROBERTSON PUPILS.
Long-standing Adie pupil: The pupil is initially dilated, but over time may constrict. Hypersensitive to pilocarpine 0.125%. SEE 10.4, ADIE (TONIC) PUPIL.
The abnormal pupil is dilated.
Iris sphincter muscle damage from trauma or surgery: Torn pupillary margin or iris transillumination defects seen on slit lamp examination.
Adie (tonic) pupil: The pupil may be irregular, reacts minimally to light, and slowly and tonically to convergence. Hypersensitive to pilocarpine 0.125%. SEE 10.4, ADIE (TONIC) PUPIL.
Third cranial nerve palsy: Always associated ptosis and/or extraocular muscle palsies. SEE 10.5, ISOLATED THIRD NERVE PALSY.
Unilateral exposure to a mydriatic agent: Cycloplegic drops (e.g., atropine), scopolamine patch for motion sickness, ill-fitting mask in patients on nebulizers (using ipratropium bromide), possible use of sympathetic medications (e.g., pseudoephedrine). If the mydriatic exposure is recent, pupil will not react to pilocarpine 1%.
Physiologic anisocoria: Pupil size disparity is the same in light as in dark, and the pupils react normally to light. The size difference is usually, but not always, <2 mm in diameter.
Work-Up
History: When was the anisocoria first noted? Associated symptoms or signs? Ocular trauma? Eye drops or ointments? Syphilis? Old photographs?
Ocular examination: Try to determine which pupil is abnormal by comparing pupil sizes in light and in dark. Anisocoria greater in light suggests the abnormal pupil is the larger pupil; anisocoria greater in dark suggests the abnormal pupil is the smaller pupil. Test the pupillary reaction to both light and near. Evaluate for the presence of a relative afferent pupillary defect. Look for ptosis, evaluate ocular motility, and examine the pupillary margin with a slit lamp.
If the abnormal pupil is small, a diagnosis of Horner syndrome may be confirmed by a cocaine or apraclonidine test (SEE 10.2, HORNER SYNDROME). In the presence of ptosis and an unequivocal increase in anisocoria in dim illumination, cocaine and apraclonidine testing may be unnecessary.
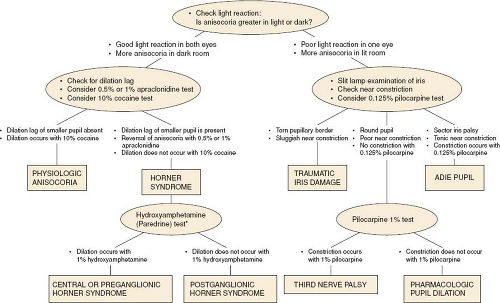
Figure 10.1.1 Flow diagram for the work-up of anisocoria. (Modified from Thompson HS, Pilley SF. Unequal pupils. A flow chart for sorting out the anisocorias. Surv Ophthalmol. 1976;21:45–48, with permission.)
*Hydroxyamphetamine should not be used within 24–48 hours of cocaine or apraclonidine to avoid possible interference with each other.
If the abnormal pupil is large and there is no sphincter muscle damage or signs of third nerve palsy (e.g., extraocular motility deficit, ptosis), the pupils are tested with one drop of pilocarpine 0.125%. Within 10 to 15 minutes, an Adie pupil will constrict significantly more than the fellow pupil (SEE 10.4, ADIE [TONIC] PUPIL).
 NOTE: For an acute Adie pupil, the pupil may not react to a weak cholinergic agent.
NOTE: For an acute Adie pupil, the pupil may not react to a weak cholinergic agent.
If the pupil does not constrict with pilocarpine 0.125%, or pharmacologic dilatation is suspected, pilocarpine 1% is instilled in both eyes. A normal pupil constricts sooner and to a greater extent than the pharmacologically dilated pupil. An eye that recently received a strong mydriatic agent such as atropine usually will not constrict at all.
10.2 Horner Syndrome
Symptoms
Ptosis and anisocoria. May have anhydrosis. Often asymptomatic.
Signs
(See Figure 10.2.1.)
Critical. Anisocoria that is greater in dim illumination (especially during the first few seconds after the room light is dimmed). The abnormal small pupil dilates less than the normal, larger pupil. Mild ptosis (2 mm) and lower eyelid elevation (“reverse ptosis”) occur on the side of the small pupil.
Other. Lower intraocular pressure, lighter iris color in congenital cases (iris heterochromia), loss of sweating (anhydrosis, distribution depends on the site of lesion), transient increase in accommodation (older patients hold their reading card closer in the Horner eye). Involved eye may have conjunctival hyperemia due to decreased episcleral vascular tone. Light and near reactions are intact.
Etiology
First-order neuron disorder: Stroke (e.g., vertebrobasilar artery insufficiency or infarct), tumor, multiple sclerosis (MS). Rarely, severe osteoarthritis of the neck with bony spurs.

Figure 10.2.1 Right Horner syndrome with ptosis and miosis.
Second-order neuron disorder: Tumor (e.g., lung carcinoma, metastasis, thyroid adenoma, neurofibroma), aortic aneurysm (e.g., tertiary syphilis). Patients with pain in the arm or scapular region should be suspected of having a Pancoast tumor. In children, consider neuroblastoma, lymphoma, or metastasis.
Third-order neuron disorder: Headache syndrome (e.g., cluster, migraine, Raeder paratrigeminal syndrome), internal carotid dissection, varicella zoster virus, otitis media, Tolosa–Hunt syndrome, neck trauma/tumor/inflammation, cavernous sinus pathology.
Congenital Horner syndrome: May also be caused by birth trauma.
Other rare causes: Cervical paraganglioma, ectopic cervical thymus.
Work-Up
Diagnosis confirmed by a relative reversal in anisocoria with apraclonidine (0.5% or 1%). The miotic pupil with Horner syndrome will appear larger than the normal pupil after apraclonidine instillation. Alternatively, 10% cocaine may be used. Place one drop of 10% cocaine in both eyes. Check in 15 minutes. If no change in pupillary size is noted, repeat drops and recheck the pupils in 15 minutes (repeat until normal pupil dilates). A Horner pupil dilates less than the normal pupil.
 NOTE: There may be a high false-negative rate to pharmacologic testing in an acute Horner syndrome.
NOTE: There may be a high false-negative rate to pharmacologic testing in an acute Horner syndrome.
A third-order neuron disorder may be distinguished from a first- and second-order neuron disorder with hydroxyamphetamine. Place one drop of 1% hydroxyamphetamine in both eyes. Check in 15 minutes and repeat if no change in pupillary size is noted. Failure of the Horner pupil to dilate to an equivalent degree as the fellow eye indicates a third-order neuron lesion, which may help guide the work-up. However, most experts feel the entire sympathetic pathway should be imaged in Horner syndrome regardless of the results of pharmacologic testing. Additionally, hydroxyamphetamine is often unavailable even from compounding pharmacies.
 NOTE: The hydroxyamphetamine test has a sensitivity of up to 93% and a specificity of 83% for identifying a third-order neuron lesion. Hydroxyamphetamine should not be used within 24–48 hours of cocaine or apraclonidine to avoid possible interference with each other. Both drops require an intact corneal epithelium and preferably no prior eye drops (including anesthetic drops) for accurate results.
NOTE: The hydroxyamphetamine test has a sensitivity of up to 93% and a specificity of 83% for identifying a third-order neuron lesion. Hydroxyamphetamine should not be used within 24–48 hours of cocaine or apraclonidine to avoid possible interference with each other. Both drops require an intact corneal epithelium and preferably no prior eye drops (including anesthetic drops) for accurate results.
Determine the duration of the Horner syndrome from the patient’s history and an examination of old photographs. New-onset Horner syndrome requires a more urgent diagnostic work-up to exclude life-threatening etiologies (e.g., internal carotid artery dissection, which can present with transient visual loss, head/neck/face pain, pulsatile tinnitus, or dysgeusia [foul taste in the mouth]). An old Horner syndrome is more likely to be benign.
History: Headaches? Arm pain? Previous stroke? Previous surgery that may have damaged the sympathetic chain, including cardiac, thoracic, thyroid, or neck surgery? History of head or neck trauma? Ipsilateral neck pain?
Physical examination (especially check for supraclavicular nodes, thyroid enlargement, or a neck mass).
Complete blood count (CBC) with differential.
Computed tomography (CT) of the chest to evaluate lung apex for possible mass (e.g., Pancoast tumor).
Magnetic resonance imaging (MRI) of the brain and neck.
Magnetic resonance angiography (MRA) or CT angiography (CTA) of head/neck to evaluate for carotid artery dissection (especially with neck pain). Obtain carotid angiogram if MRA or CTA yield equivocal results.
Lymph node biopsy when lymphadenopathy is present.
Treatment
Treat the underlying disorder if possible.
 NOTE: Carotid dissection usually requires antiplatelet therapy to prevent carotid occlusion and hemispheric stroke in consultation with neurology and neurosurgery. Anticoagulation is occasionally used. Rarely, ischemic symptoms in the distribution of the dissection persist despite antiplatelet therapy. In these cases, surgical intervention may be considered.
NOTE: Carotid dissection usually requires antiplatelet therapy to prevent carotid occlusion and hemispheric stroke in consultation with neurology and neurosurgery. Anticoagulation is occasionally used. Rarely, ischemic symptoms in the distribution of the dissection persist despite antiplatelet therapy. In these cases, surgical intervention may be considered.
Ptosis surgery may be performed electively.
Follow-Up
Work-up acute Horner syndromes as soon as possible to rule out life-threatening causes. Neuroimaging (as above) should be performed immediately for dissection. Remaining workup may be performed within 1 to 2 days.
Chronic Horner syndrome can be evaluated with less urgency. There are no ocular complications that necessitate close follow-up.
10.3 Argyll Robertson Pupils
Symptoms
Usually asymptomatic.
Signs
Critical. Small, irregular pupils that exhibit “light-near” dissociation (react poorly or not at all to light but constrict normally during convergence). By definition, vision must be intact.
Other. The pupils dilate poorly in darkness. Always bilateral, although may be asymmetric.
Differential Diagnosis of “Light-Near” Dissociation
Bilateral optic neuropathy or severe retinopathy: Reduced visual acuity with normal pupil size.
Adie (tonic) pupil: Unilateral or bilateral irregularly dilated pupil that constricts slowly and unevenly to light. Normal vision. SEE 10.4, ADIE (TONIC) PUPIL.
Dorsal midbrain (Parinaud) syndrome: Associated with eyelid retraction (Collier sign), supranuclear upgaze palsy, and convergence retraction nystagmus. SEE 10.4, ADIE (TONIC) PUPIL AND “CONVERGENCE-RETRACTION” IN 10.21, NYSTAGMUS.
Rarely caused by third nerve palsy with aberrant regeneration. SEE 10.6, ABERRANT REGENERATION OF THE THIRD NERVE.
Others: Diabetes, alcoholism, etc.
Etiology
Tertiary syphilis.
Work-Up
Test the pupillary reaction to light and convergence: To test the reaction to convergence, patients are asked to look first at a distant target and then at their own finger, which the examiner holds in front of them and slowly brings in toward their face.
Slit lamp examination: Look for interstitial keratitis (SEE 4.17, INTERSTITIAL KERATITIS).
Dilated fundus examination: Search for chorioretinitis, papillitis, and uveitis.
Fluorescent treponemal antibody absorption (FTA-ABS) or treponemal-specific assay (e.g., microhemagglutination assay – Treponema pallidum [MHA-TP]), and rapid plasma reagin (RPR) or Venereal Disease Research Laboratory (VDRL) test.
If the diagnosis of syphilis is established, lumbar puncture (LP) may be indicated. SEE 12.12, SYPHILIS, for specific indications.
Treatment
Treatment based on the presence of active disease and previous appropriate treatment.
SEE 12.12, SYPHILIS, for treatment indications and specific antibiotic therapy.
Follow-Up
Pupillary findings alone are not an emergency. Diagnostic work-up and determination of syphilitic activity should be undertaken within a few days.
10.4 Adie (Tonic) Pupil
Symptoms
Difference in size of pupils, blurred near vision, photophobia. May be asymptomatic.
Signs
Critical. An irregularly dilated pupil that has minimal or no reactivity to light. Slow, tonic constriction with convergence, and slow redilation. May have vermiform iris movement and/or sectoral iris sphincter paresis.
Other. May have an acute onset and become bilateral. The involved pupil may become smaller than the normal pupil over time.
Differential Diagnosis
SEE 10.1, ANISOCORIA.
Parinaud syndrome/dorsal midbrain lesion: Bilateral mid-dilated pupils that react poorly to light but constrict normally with convergence (not tonic). Associated with eyelid retraction (Collier sign), supranuclear upgaze paralysis, and convergence retraction nystagmus. An MRI should be performed to rule out pinealoma and other midbrain pathology.
Holmes–Adie syndrome: Tonic pupil and tendon areflexia. May be associated with autonomic and peripheral neuropathy.
Argyll Robertson Pupils: SEE 10.3, ARGYLL ROBERTSON PUPILS.
Etiology
Idiopathic most commonly. Orbital trauma, surgery, and varicella zoster infection are seen frequently. Early syphilis, parvovirus B19, herpes simplex virus, botulism, paraneoplastic syndrome, giant cell arteritis (GCA), pan-retinal photocoagulation, and neurologic Lyme disease less commonly.
Rare associations reported with endometriosis, seminomas, and Sjögren syndrome.
Rare associations reported with endometriosis, seminomas, and Sjögren syndrome.
Work-Up
SEE 10.1, ANISOCORIA, for a general work-up when the diagnosis is uncertain.
Evaluate pupils and iris at slit lamp or with a muscle light for irregular slow constriction or abnormal movement.
Test for cholinergic hypersensitivity. Instill 0.125% pilocarpine in both eyes and recheck pupils in 10 to 15 minutes. An Adie pupil constricts while the normal pupil does not.
If bilateral simultaneous Adie pupils, consider further laboratory investigations including testing for the aforementioned etiologies. For unilateral involvement, no further laboratory investigations are necessary.
 NOTE: The dilute pilocarpine test may occasionally be positive in familial dysautonomia. Hypersensitivity may not be present with an acute Adie pupil and may need to be retested a few weeks later.
NOTE: The dilute pilocarpine test may occasionally be positive in familial dysautonomia. Hypersensitivity may not be present with an acute Adie pupil and may need to be retested a few weeks later.
If Adie pupil is present in a patient younger than 1 year, consult a pediatric neurologist to rule out familial dysautonomia (Riley–Day syndrome).
Treatment
Pilocarpine 0.125% b.i.d. to q.i.d. may be considered for cosmesis and to aid in accommodation.
Follow-Up
If the diagnosis is certain, follow-up is routine.
Symptoms
Binocular diplopia and ptosis; with or without pain.
Signs
(See Figures 10.5.1 to 10.5.4.)
Critical
External ophthalmoplegia.
Complete palsy: Limitation of ocular movement in all fields of gaze except temporally.

Figure 10.5.1 Isolated right third cranial nerve palsy with complete ptosis.

Figure 10.5.2 Isolated right third cranial nerve palsy: Primary gaze showing right exotropia and dilated pupil.

Figure 10.5.3 Isolated right third cranial nerve palsy: Left gaze showing inability to adduct right eye.
Figure 10.5.4 Isolated right third cranial nerve palsy: Right gaze showing normal abduction of right eye.
Incomplete palsy: Partial limitation of ocular movement.
Superior division palsy: Ptosis and an inability to look up.
Inferior division palsy: Inability to look nasally or inferiorly.
Internal ophthalmoplegia.
Pupil-involving: A fixed, dilated, poorly reactive pupil.
Pupil-sparing: Pupil not dilated and normally reactive to light.
Relative pupil-sparing: Pupil partially dilated and sluggishly reactive to light.
Other. An exotropia or hypotropia. Aberrant regeneration. SEE 10.6, ABERRANT REGENERATION OF THE THIRD NERVE.
Differential Diagnosis
Myasthenia gravis: Diurnal variation of symptoms and signs, pupil never involved, increased eyelid droop after sustained upgaze. SEE 10.11, MYASTHENIA GRAVIS.
Thyroid eye disease: Eyelid lag, lid retraction, injection over the rectus muscles, proptosis, positive forced duction testing. SEE 7.2.1, THYROID EYE DISEASE.
Chronic progressive external ophthalmoplegia (CPEO): Bilateral, slowly progressive ptosis and motility limitation. Pupil spared, often no diplopia. SEE 10.12, CHRONIC PROGRESSIVE EXTERNAL OPHTHALMOPLEGIA.
Idiopathic orbital inflammatory syndrome: Pain and proptosis common. SEE 7.2.2, IDIOPATHIC ORBITAL INFLAMMATORY SYNDROME.
Internuclear ophthalmoplegia (INO): Unilateral or bilateral adduction deficit with horizontal nystagmus of opposite abducting eye. No ptosis. SEE 10.13, INTERNUCLEAR OPHTHALMOPLEGIA.
Skew deviation: Supranuclear brainstem lesion producing asymmetric, mainly vertical ocular deviation not consistent with single cranial nerve defect. SEE DIFFERENTIAL DIAGNOSIS IN 10.7, ISOLATED FOURTH NERVE PALSY.
Parinaud syndrome/dorsal midbrain lesion: Bilateral mid-dilated pupils that react poorly to light but constrict normally with convergence (not tonic). Associated with eyelid retraction (Collier sign), supranuclear upgaze paralysis, and convergence retraction nystagmus. No ptosis.
GCA: Extraocular muscle ischemia due to involvement of the long posterior ciliary arteries. Any extraocular muscle may be affected, resulting in potentially complex horizontal and vertical motility deficits. Pupil typically not involved. Age ≥55 years. SEE 10.17, ARTERITIC ISCHEMIC OPTIC NEUROPATHY (GIANT CELL ARTERITIS).
Etiology
Pupil-involving:
More common: Aneurysm, particularly posterior communicating artery aneurysm.
Less common: Tumor, trauma, congenital, uncal herniation, cavernous sinus mass lesion, pituitary apoplexy, orbital disease, varicella zoster virus, ischemia (e.g., diabetic), and leukemia. In children, ophthalmoplegic migraine.
Pupil-sparing: Ischemic microvascular disease; rarely cavernous sinus syndrome or GCA.
Relative pupil-sparing: Ischemic microvascular disease; less likely compressive.
Aberrant regeneration present: Trauma, aneurysm, tumor, congenital. Not microvascular. SEE 10.6, ABERRANT REGENERATION OF THE THIRD NERVE.
Work-Up
History: Onset and duration of diplopia? Recent trauma? Pertinent medical history (e.g., diabetes, hypertension, known cancer or central nervous system mass, recent infections). If ≥55 years old, ask specifically about GCA symptoms.
Complete ocular examination: Check for pupillary involvement, the directions of motility restriction (in both eyes), ptosis, a visual
field defect (visual fields by confrontation), proptosis, resistance to retropulsion, orbicularis muscle weakness, and eyelid fatigue with sustained upgaze. Look carefully for signs of aberrant regeneration. SEE 10.6, ABERRANT REGENERATION OF THE THIRD NERVE.
Neurologic examination: Carefully assess the other cranial nerves on both sides.
 NOTE: The ipsilateral fourth nerve can be assessed by focusing on a superior conjunctival blood vessel and asking the patient to look down. The eye should intort, and the blood vessel should turn down and toward the nose even if the eye cannot be adducted.
NOTE: The ipsilateral fourth nerve can be assessed by focusing on a superior conjunctival blood vessel and asking the patient to look down. The eye should intort, and the blood vessel should turn down and toward the nose even if the eye cannot be adducted.
Immediate CNS imaging to rule out mass/aneurysm is indicated for all third nerve palsies whether pupil-involving or pupil-sparing. One possible exception is a patient with complete sparing of the pupil and complete involvement of the other muscles (i.e., complete ptosis and complete paresis of extraocular muscles innervated by cranial nerve three).
 NOTE: Most sensitive modality is contrast-enhanced CT and CTA, though gadolinium-enhanced MRI and MRA are also very sensitive and can be done if CT and CTA are contraindicated or unavailable. Choice of imaging should be made in conjunction with neuroradiology. If initial imaging studies are negative but clinical suspicion remains high, catheter angiography may be indicated.
NOTE: Most sensitive modality is contrast-enhanced CT and CTA, though gadolinium-enhanced MRI and MRA are also very sensitive and can be done if CT and CTA are contraindicated or unavailable. Choice of imaging should be made in conjunction with neuroradiology. If initial imaging studies are negative but clinical suspicion remains high, catheter angiography may be indicated.
Cerebral angiography is indicated for all patients >10 years of age with pupil-involving third nerve palsies and whose imaging study is not definitively negative or shows a mass consistent with an aneurysm.
CBC with differential in children.
Ice test, rest test, or edrophonium chloride test when myasthenia gravis is suspected. SEE 10.11, MYASTHENIA GRAVIS.
For suspected ischemic disease: Check blood pressure, fasting blood sugar, hemoglobin A1c.
Immediate erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), and platelets if GCA is suspected. SEE 10.17, ARTERITIC ISCHEMIC OPTIC NEUROPATHY (GIANT CELL ARTERITIS).
Treatment
Treat the underlying abnormality.
If the third nerve palsy is causing symptomatic diplopia, an occlusion patch or prism may be placed over the involved eye. Patching is usually not performed in children <11 years of age because of the risk of amblyopia. Children should be monitored closely for the development of amblyopia in the deviated eye.
Strabismus surgery may be considered for persistent significant misalignment.
Follow-Up
Follow-up intervals vary depending on underlying disorder and stability of examination findings. Comanagement with medicine, neurosurgery, and/or neurology may be necessary.
If secondary to ischemia, function should return within 3 months. Refer to internist for management of vasculopathic disease risk factors.
If pupil-involving and imaging/angiography are negative, an LP should be considered.
10.6 Aberrant Regeneration of the Third Nerve
Signs
(See Figures 10.6.1 and 10.6.2.)
The most common signs of aberrant third nerve regeneration include:
Eyelid-gaze dyskinesis: Elevation of involved eyelid on downgaze (Pseudo-von Graefe sign) or adduction.
Pupil-gaze dyskinesis: Pupil constricts on downgaze or adduction.
 Figure 10.6.1 Aberrant regeneration of right third cranial nerve showing right-sided ptosis in primary gaze. |
 Figure 10.6.2 Aberrant regeneration of right third cranial nerve showing right upper eyelid retraction on attempted left gaze. |
Etiology
Thought to result from misdirection of the third nerve fibers from their original destination to alternate third nerve controlled muscles (e.g., inferior rectus to the pupil).
Aberrancy from congenital third nerve palsies: Can be seen in up to two-thirds of these patients.
Aberrancy from prior acquired third nerve palsies: Seen most often in patients recovering from third nerve damage by trauma or compression by a posterior communicating artery aneurysm.
Primary aberrant regeneration: A term used to describe the presence of aberrant regeneration in a patient who has no history of a third nerve palsy. Usually indicates the presence of a progressively enlarging parasellar lesion such as a carotid aneurysm or meningioma within the cavernous sinus.
Work-Up
Aberrancy from congenital: None. Document work-up of prior congenital third nerve palsy.
Aberrancy from acquired: SEE 10.5, ISOLATED THIRD NERVE PALSY. Document work-up of prior acquired third nerve palsy if previously obtained.
Primary aberrancy: All patients must undergo neuroimaging to rule out slowly compressive lesion or aneurysm.
Treatment
Treat the underlying disorder.
Consider strabismus surgery if significant symptoms are present.
Follow-Up
Aberrancy from congenital: Routine.
Aberrancy from acquired: As per the underlying disorder identified in the work-up.
Primary aberrancy: As per neuroimaging and clinical examination findings. Patients are instructed to return immediately for any changes (e.g., ptosis, diplopia, sensory abnormality).
Symptoms
Binocular vertical (or oblique) diplopia, difficulty reading, sensation that objects appear tilted; may be asymptomatic.
Signs
(See Figures 10.7.1 and 10.7.2.)
Critical. Deficient inferior movement of an eye when attempting to look down and in.
The three-step test isolates a palsy of the superior oblique muscle (see #3 under Work-up, Perform the three-step test).
The three-step test isolates a palsy of the superior oblique muscle (see #3 under Work-up, Perform the three-step test).
 Figure 10.7.1 Isolated left fourth cranial nerve palsy: Primary gaze showing left hypertropia. |
Other. The involved eye is higher (hypertropic) in primary gaze. The hypertropia increases when looking in the direction of the uninvolved eye or tilting the head toward the ipsilateral shoulder. The patient often maintains a head tilt toward the contralateral shoulder to eliminate diplopia.
Differential Diagnosis
All of the following may produce binocular vertical diplopia, hypertropia, or both.
Myasthenia gravis: Variable symptoms with fatigability. Ptosis common. Orbicularis oculi weakness often present. SEE 10.11, MYASTHENIA GRAVIS.
Thyroid eye disease: May have proptosis, eyelid lag, lid retraction, or injection over the involved rectus muscles. Positive forced duction test. SEE 7.2.1, THYROID EYE DISEASE AND APPENDIX 6, FORCED DUCTION TEST AND ACTIVE FORCE GENERATION TEST.

Figure 10.7.2 Isolated left fourth cranial nerve palsy: Right gaze with left inferior oblique overaction.
Idiopathic orbital inflammatory syndrome: Pain and proptosis are common. SEE 7.2.2, IDIOPATHIC ORBITAL INFLAMMATORY SYNDROME.
Orbital fracture: History of trauma. Positive forced duction test. SEE 3.9, ORBITAL BLOWOUT FRACTURE.
Skew deviation: The three-step test does not isolate a particular muscle. Rule out a posterior fossa or brainstem lesion with neuroimaging. SEE 10.13, INTERNUCLEAR OPHTHALMOPLEGIA.
Incomplete third nerve palsy: Inability to look down and in, usually with adduction weakness. Intorsion on attempted downgaze. Three-step test does not isolate the superior oblique. SEE 10.5, ISOLATED THIRD NERVE PALSY.
Brown syndrome: Limitation of elevation in adduction due to restriction of superior oblique tendon. May be congenital or acquired (e.g., trauma, inflammation). Positive forced duction test. SEE 8.6, STRABISMUS SYNDROMES.
GCA: Extraocular muscle ischemia causing nonspecific motility deficits or neural ischemia mimicking a cranial nerve palsy. Age ≥55 years, usually associated systemic symptoms. SEE 10.17, ARTERITIC ISCHEMIC OPTIC NEUROPATHY (GIANT CELL ARTERITIS).
Etiology
More Common. Trauma, vascular infarct (often the result of underlying diabetes or hypertension), congenital, idiopathic, or demyelinating disease.
Rare. Tumor, hydrocephalus, aneurysm, GCA.
Work-Up
History: Onset and duration of the diplopia? Misaligned eyes or head tilt since early childhood? Trauma? Stroke?
Examine old photographs to determine whether the head tilt is long-standing, indicating a chronic or congenital fourth nerve palsy.
Perform the three-step test:
Step 1: Determine which eye is deviated upward in primary gaze. This is best seen with the cover–uncover test (SEE APPENDIX 3, COVER/UNCOVER AND ALTERNATE COVER TESTS). The higher eye comes down after being uncovered.
Step 2: Determine whether the upward deviation is greater when the patient looks to the left or to the right.
Step 3: Determine whether the upward deviation is greater when tilting the head to the left shoulder or right shoulder.
Patients with a superior oblique muscle paresis have a hyperdeviation that is worse on contralateral gaze and when tilting the head toward the shoulder ipsilateral to the affected eye.
In addition to the findings on the three-step test, the hypertropia should be greater in downgaze than in upgaze.
Patients with bilateral fourth nerve palsies demonstrate hypertropia of the right eye when looking left, hypertropia of the left eye when looking right, and a “V”-pattern esotropia (the eyes cross more when looking down due to a decrease of the abducting effect of the superior oblique muscles in depression as well as overaction of the inferior oblique muscles).
Perform the double Maddox rod test if bilateral fourth nerve palsies are suspected to measure total excyclotorsion.
A white Maddox rod is placed before one eye and a red Maddox rod is placed before the other eye in a trial frame or phoropter, aligning the axes of each rod along the 90 degrees vertical mark. While looking at a white light in the distance, the patient is asked if both the white and red lines seen through the Maddox rods are horizontal and parallel to each other. If not, the patient is asked to rotate the Maddox rod(s) until they are parallel. If he or she rotates the top of this vertical axis outward (away from the nose) for more than 10 degrees total for the two eyes, then a bilateral superior oblique muscle paresis is likely present.
 NOTE: The double Maddox rod test (or variations thereof) can be used to evaluate any suspected underlying strabismus and can help the practitioner measure ocular misalignment and subtle deviations.
NOTE: The double Maddox rod test (or variations thereof) can be used to evaluate any suspected underlying strabismus and can help the practitioner measure ocular misalignment and subtle deviations.
Measure vertical fusional amplitudes with a vertical prism bar to distinguish a congenital from an acquired palsy.
A patient with an acquired fourth nerve palsy has a normal vertical fusional amplitude of 6 prism diopters or less. A patient with a congenital fourth nerve palsy has greater than 6 prism diopters of fusional amplitude.
Ice test, rest test, or less commonly edrophonium chloride test if myasthenia gravis is suspected (SEE 10.11, MYASTHENIA GRAVIS).
CT scan of head and orbits (axial, coronal, and parasagittal views) for suspected orbital disease.
Blood pressure measurement, fasting blood sugar, and hemoglobin A1c. Immediate ESR, CRP, and platelets if GCA is suspected.
MRI of the brain for:
A fourth nerve palsy accompanied by other cranial nerve or neurologic abnormalities.
All patients <45 years of age with no history of significant head trauma, and patients aged 45 to 55 years with no vasculopathic risk factors or trauma.
Treatment
Treat the underlying disorder.
An occlusion patch may be placed over one eye or fogging plastic tape can be applied to one lens of patient’s spectacles to relieve symptomatic double vision. Patching is usually not performed in children <11 years of age because of the risk of amblyopia.
Prisms in spectacles may be prescribed for small, stable hyperdeviations.
Strabismus surgery may be indicated for bothersome double vision in primary or reading position or for a cosmetically significant head tilt. Defer surgery for at least 6 months after onset of the palsy to allow for deviation stabilization or possible spontaneous resolution.
Follow-Up
Congenital fourth nerve palsy: Routine.
Acquired fourth nerve palsy: As per the underlying disorder. If the work-up is negative, the lesion is presumed vascular or idiopathic and the patient is reexamined in 1 to 3 months. If the palsy does not resolve in 3 months or if an additional neurologic abnormality develops, appropriate imaging studies of the brain are indicated. Patients are instructed to return immediately for any changes (e.g., ptosis, worsening diplopia, sensory abnormality, pupil abnormality).
Symptoms
Binocular horizontal diplopia, worse for distance than near, most pronounced in the direction of the paretic lateral rectus muscle.
Signs
(See Figures 10.8.1 and 10.8.2.)
Critical. Deficient lateral movement of an eye with negative forced duction testing (SEE APPENDIX 6, FORCED DUCTION TEST AND ACTIVE FORCE GENERATION TEST).
Other. No proptosis.
Differential Diagnosis of Limited Abduction
Thyroid eye disease: May have proptosis, eyelid lag, lid retraction, injection over the involved rectus muscles, and positive forced duction testing. SEE 7.2.1, THYROID EYE DISEASE.
Myasthenia gravis: Variable symptoms with fatigability. Ptosis common. Positive ice test, rest test, or less commonly edrophonium chloride test. SEE 10.11, MYASTHENIA GRAVIS.
Idiopathic orbital inflammatory syndrome: Pain and proptosis are common. SEE 7.2.2, IDIOPATHIC ORBITAL INFLAMMATORY SYNDROME.
Orbital trauma: Fracture causing medial rectus entrapment, positive forced duction testing. SEE 3.9, ORBITAL BLOWOUT FRACTURE.
Duane syndrome, type 1: Congenital; narrowing of the palpebral fissure and retraction of the globe on adduction. SEE 8.6, STRABISMUS SYNDROMES.

Figure 10.8.1 Isolated right sixth cranial nerve palsy: Left gaze showing full adduction.
Möbius syndrome: Congenital; bilateral facial paralysis present. SEE 8.6, STRABISMUS SYNDROMES.
Convergence spasm: Intermittent, variable episodes of convergence and miosis. May appear to have abduction deficit when assessing versions, however ductions are full. Miotic pupils help to differentiate since pupils are not affected in an isolated sixth nerve palsy.
Primary divergence insufficiency: Usually acquired and benign; esotropia and diplopia only at distance and single binocular vision at near. Symptoms may improve spontaneously without treatment or may be corrected with base-out prisms or surgery. If the history reveals sudden onset, trauma, infection (e.g., meningitis, encephalitis), MS, or malignancy, divergence paralysis should be considered and a neurologic work-up with MRI of the brain and brainstem obtained.
GCA: Less common, however may occur with extraocular muscle ischemia; in patients age ≥55 years. May be associated with systemic symptoms. SEE 10.17, ARTERITIC ISCHEMIC OPTIC NEUROPATHY (GIANT CELL ARTERITIS).
Etiology
Adults
More Common. Vasculopathic (e.g., diabetes, hypertension, other atherosclerotic risk factors), trauma, idiopathic.
Less Common. Increased intracranial pressure, cavernous sinus mass (e.g., meningioma, aneurysm, metastasis), MS, sarcoidosis, vasculitis, after myelography or LP, stroke (usually with other neurologic deficits), meningeal inflammation/infection (e.g., Lyme disease, neurosyphilis), GCA.
 Figure 10.8.2 Isolated right sixth cranial nerve palsy: Right gaze showing limited abduction. |
Children
Benign and usually self-limited after viral infection or vaccination, trauma, increased intracranial pressure (e.g., obstructive hydrocephalus), pontine glioma, Gradenigo syndrome (petrositis causing sixth and often seventh nerve involvement, with or without eighth and fifth nerve involvement on the same side; associated with complicated otitis media).
Work-Up
Adults
History: Do the symptoms fluctuate during the day? Cancer, diabetes, or thyroid disease? Symptoms of GCA (in the appropriate age group)?
Complete neurologic and ophthalmic examinations; pay careful attention to the function of the other cranial nerves and the appearance of the optic disc. Because of the risk of corneal damage, it is especially important to evaluate the fifth cranial nerve. Corneal sensation (supplied by the first division) can be tested by touching a wisp of cotton or a tissue to the corneas before applying topical anesthetic. Ophthalmoscopy looking for papilledema is required because increased intracranial pressure from any cause can result in unilateral or bilateral sixth nerve palsies.
Check blood pressure, fasting blood sugar, and hemoglobin A1c.
MRI of the brain is indicated for the following patients:
Younger than 45 years of age (if MRI is negative, consider LP).
Patients aged 45 to 55 years with no vasculopathic risk factors.
Sixth nerve palsy accompanied by severe pain or any other neurologic or neuro-ophthalmic signs.
Any history of cancer.
Bilateral sixth nerve palsies.
Papilledema is present.
Immediate ESR, CRP, and platelet count if GCA is suspected. SEE 10.17, ARTERITIC ISCHEMIC OPTIC NEUROPATHY (GIANT CELL ARTERITIS).
Consider Lyme antibody as well as FTA-ABS or treponemal-specific assay and RPR or VDRL tests.
Children
History: Recent illness or trauma? Neurologic symptoms, lethargy, or behavioral changes? Chronic ear infections?
Complete neurologic and ophthalmic examinations as described for adults.
Otoscopic examination to rule out complicated otitis media.
MRI of the brain in all children.
Treatment
Treat any underlying problem revealed by the work-up.
An occlusion patch may be placed over one eye or fogging plastic tape applied to one spectacle lens to relieve symptomatic diplopia. In patients <11 years, patching is avoided, and these patients are monitored closely for the development of amblyopia. SEE 8.7, AMBLYOPIA.
Prisms in glasses may be fit acutely for temporary relief or for chronic stable deviations (e.g., after stroke). Consider strabismus surgery for a stable deviation that persists >6 months.
Follow-Up
Reexamine every 6 weeks after the onset of the palsy until it resolves. MRI of the head is indicated if any new neurologic signs or symptoms develop, the abduction deficit increases, or the isolated sixth nerve palsy does not resolve in 3 to 6 months.
10.9 Isolated Seventh Nerve Palsy
Symptoms
Weakness or paralysis of one side of the face, inability to close one eye, excessive drooling.
Signs
(See Figures 10.9.1 and 10.9.2.)
Critical. Unilateral weakness or paralysis of the facial musculature.
Central lesion: Weakness or paralysis of lower facial musculature only. Upper eyelid closure and forehead wrinkling intact.
Peripheral lesion: Weakness or paralysis of upper and lower facial musculature.
 Figure 10.9.1 Isolated peripheral left seventh cranial nerve palsy demonstrating lagophthalmos. |
 Figure 10.9.2 Isolated peripheral left seventh cranial nerve palsy demonstrating paralysis of upper facial muscles. |
Other. Flattened nasolabial fold, droop of corner of the mouth, ectropion, and lagophthalmos. May have ipsilateral decreased taste on anterior two-thirds of tongue, decreased basic tear production, or hyperacusis. May have an injected eye with a corneal epithelial defect. Synkinesis, a simultaneous movement of muscles supplied by different branches of the facial nerve or simultaneous stimulation of visceral efferent fibers of facial nerve (e.g., corner of mouth contracts when eye closes, excessive lacrimation when eating [“crocodile” tears]), secondary to aberrant regeneration implying chronicity.
Etiology
Central Lesions
Cortical: Lesion of contralateral motor cortex or internal capsule (e.g., stroke, tumor). Loss of voluntary facial movement; emotional facial movement sometimes intact. May also have ipsilateral hemiparesis.
Extrapyramidal: Lesion of basal ganglia (e.g., parkinsonism, tumor, vascular lesion of basal ganglia). Loss of emotional facial movement; volitional facial movement intact. Not a true facial paralysis.
Brainstem: Lesion of ipsilateral pons (e.g., MS, stroke, tumor). Often with ipsilateral sixth nerve palsy, contralateral hemiparesis. Occasionally with cerebellar signs.
Peripheral Lesions
Cerebellopontine angle (CPA) masses (e.g., acoustic neuroma, facial neuroma, meningioma, cholesteatoma, metastasis): Gradual progressive onset, although sometimes acute. May have facial pain, twitching, or a characteristic nystagmus. This is small-amplitude rapid jerk nystagmus in which the fast phase is directed away from the side of the lesion (peripheral vestibular) in conjunction with a slow, gaze-evoked nystagmus directed toward the side of the lesion (from brainstem compression). May have eighth nerve dysfunction, including hearing loss, tinnitus, vertigo, or dysequilibrium.
Temporal bone fracture: History of head trauma. May have Battle sign (ecchymoses over mastoid region), cerebrospinal fluid otorrhea, hearing loss, vertigo, or vestibular nystagmus.
Other trauma: Accidental or iatrogenic (e.g., facial laceration, local anesthetic block, parotid or mastoid surgery).
Acute or chronic suppurative otitis media.
Malignant otitis externa: Pseudomonas infection in diabetic or elderly patients. Begins in external auditory canal but may progress to osteomyelitis, meningitis, or abscess.
Ramsay–Hunt syndrome (varicella zoster oticus): Viral prodrome followed by ear pain; vesicles on pinna, external auditory canal, tongue, face, or neck. Progresses over 10 days. May have sensorineural hearing loss, tinnitus, or vertigo.
Guillain–Barré syndrome: Viral syndrome followed by progressive motor weakness or paralysis or cranial nerve palsies, or both. Loss of deep tendon reflexes. May have bilateral facial palsies.
Lyme disease: May have rash, fever, fatigue, arthralgias, myalgias, or nausea. There may or may not be a history of tick bite. SEE 13.3, LYME DISEASE.
Sarcoidosis: May have uveitis, parotitis, skin lesions, or lymphadenopathy. May have bilateral facial palsies. SEE 12.6, SARCOIDOSIS.
Parotid neoplasm: Slowly progressive paralysis of all or portion of facial musculature. Parotid mass with facial pain.
Metastasis: History of primary tumor (e.g., breast, lung, prostate). Multiple cranial nerve palsies in rapid succession may be seen. Can be the result of basilar skull metastasis or carcinomatous meningitis.
Bell palsy: Idiopathic seventh nerve palsy. Most common, but other etiologies must be ruled out. May have viral prodrome followed by ear pain, facial numbness, decreased tearing or taste. Facial palsy may be complete or incomplete and progress over 10 days. May be recurrent, rarely bilateral. Possible familial predisposition.
Others: Diabetes mellitus, botulism, human immunodeficiency virus (HIV), syphilis, Epstein–Barr virus, acute porphyrias, nasopharyngeal carcinoma, collagen–vascular disease, and others.
Work-Up
History: Onset and duration of facial weakness? First episode or recurrence? Facial or ear pain? Trauma? Stroke? Recent infection? Hearing loss, tinnitus, dizziness, or vertigo? History of sarcoidosis or cancer?
Examine old photographs to determine chronicity of facial droop.
Complete neurologic examination: Determine if facial palsy is central or peripheral, complete or incomplete. Look for motor weakness and cerebellar signs. Carefully assess other cranial nerves, especially the fifth, sixth, and seventh. Consider assessing taste on anterior two-thirds of tongue on affected side.
Complete ocular examination: Check ocular motility and look for nystagmus. Assess orbicularis strength bilaterally, degree of ectropion, and Bell phenomenon. Examine cornea carefully for signs of exposure (superficial punctate keratopathy, epithelial defect, or ulcer). Perform Schirmer test (SEE 4.3, DRY EYE SYNDROME) to assess basic tear production. Check for signs of uveitis.
Otolaryngologic examination: Examine ear and oropharynx for vesicles, masses, or other lesions. Palpate parotid for mass or lymphadenopathy. Check hearing.
CT scan if history of trauma to rule out basilar skull fracture: Axial, coronal, and parasagittal cuts with attention to temporal bone.
MRI or CT scan of brain if any other associated neurologic signs, history of cancer, or duration >3 months. Sixth nerve involvement warrants attention to the brainstem. Eighth nerve involvement warrants attention to the CPA. Multiple cranial nerve involvement warrants attention to the skull base and cavernous sinus.
CT chest or chest radiograph and angiotensin-converting enzyme (ACE) level if sarcoidosis suspected.
Consider CBC with differential, Lyme antibody, Epstein–Barr virus titer, HIV test, FTA-ABS or treponemal-specific assay and RPR or VDRL tests depending on suspected etiology.
Consider rheumatoid factor, ESR, antinuclear antibody (ANA), and antineutrophil cytoplasmic antibody if collagen–vascular disease suspected.
Echocardiogram, Holter monitor, carotid noninvasive studies in patients with a history of stroke.
LP in patients with history of primary neoplasm to rule out carcinomatous meningitis (may repeat if negative to increase sensitivity).
Treatment
Treat the underlying disease as follows:
Stroke: Refer to neurologist.
CPA masses, temporal bone fracture, nerve laceration: Refer to neurosurgeon.
Otitis: Refer to otolaryngologist.
Ramsay–Hunt syndrome: If seen within 72 hours of onset, start acyclovir 800 mg five times per day for 7 to 10 days (contraindicated in pregnancy and renal failure). Refer to otolaryngologist.
Guillain–Barré syndrome: Refer to neurologist. May require urgent hospitalization for rapidly progressive motor weakness or respiratory distress.
Lyme disease: Refer to infectious disease specialist. May need LP. Treat with oral doxycycline, penicillin, or intravenous (i.v.) ceftriaxone. SEE 13.3, LYME DISEASE.
Sarcoidosis: Treat uveitis if present. Consider brain MRI, LP, or both to rule out CNS involvement; if present, refer to neurologist. Refer to internist for systemic evaluation. May require systemic prednisone for extraocular or CNS disease. SEE 12.6, SARCOIDOSIS.
Metastatic disease: Refer to oncologist. Systemic chemotherapy, radiation, or both may be required.
Bell palsy: 86% of patients recover completely with observation alone within 2 months. Options for treatment include:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


