Neuro-Ophthalmic Disease
Pupil Abnormalities
Leonid Skorin Jr
Bruce G. Muchnick
ICD-9: 379.40
THE DISEASE
Pathophysiology
Pupil size reflects the neural input of both the sympathetic and parasympathetic systems on the dilator and sphincter muscles, respectively, of the iris. Normal pupils are 3 to 4 mm in diameter in ambient light and are relatively equal in size. This equality in pupil size is a result of the bilateral symmetrical afferent input to the Edinger-Westphal complex in the midbrain and because of the symmetrical output of the paired sympathetic nuclei in the hypothalamus. Any disruption of the neural pathway or iris architecture will lead to abnormalities of the pupillary state.
Etiology
Arelative afferent pupillary deficit (RAPD) or Marcus Gunn pupil will result from a significant unilateral or asymmetric visual deficit caused by retinal or optic nerve disease (optic neuropathy).
Anisocoria is the state where the two pupils are unequal in size. The etiology depends on whether the abnormal pupil is the dilated or constricted pupil.
Dilated pupils can occur from iris sphincter trauma, Adie’s tonic pupil, third-nerve palsy, or pharmacologic blockade. Constricted pupils can occur with iritis, pharmacologic blockade, Horner’s syndrome, Argyll Robertson pupil, or long-standing Adie’s pupil.
Physiologic anisocoria is present when the pupil size difference remains the same in both bright light and in darkness.
The Patient
Symptoms and signs will vary according to the underlying etiology.
Clinical Symptoms
Patients with a RAPD will complain of vision and color loss in the affected eye.
Patients with anisocoria are often asymptomatic or may complain of other symptoms, such as droopy eyelid, blurred vision, focusing problems, or diplopia, depending on any accompanying symptoms.
Clinical Signs
Prominent Signs
With RAPD, there will be a positive swinging flashlight test (Fig. 19-1).
Anisocoria—Pupillary size difference that may vary between light and dark.
Adie’s tonic pupil—The affected pupil is larger and reacts poorly to light or near stimuli.
Argyll Robertson pupil—The miotic pupils are irregular and do not respond to light with poor dilation in the dark yet good near response.
Pharmacologic pupil—Either miotic or dilated pupil that does not respond to any pharmacologic testing.
Horner’s syndrome—Miotic pupil accompanied by ptosis and possibly anhidrosis. Anhidrosis will be present if the lesion involves the sympathetic pathway proximal to the bifurcation of the common carotid artery.
Third-nerve palsy—Dilated pupil accompanied by ptosis and extraocular muscle palsies.
In light-near dissociation (LND) of pupils, there is better pupillary response to near stimuli than to light stimuli. This is found in optic neuropathy, retinopathy, Adie’s tonic pupil, Argyll Robertson pupil, Parinaud’s dorsal midbrain syndrome, aberrant regeneration of the third nerve, and diabetes.
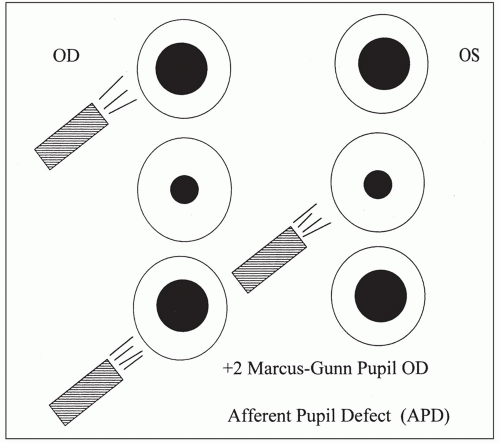 Figure 19-1. Swinging flashlight test (examiner facing patient). Right eye affected; left eye normal. Illustration courtesy of Kathleen A. Skorin, C.O.A. |
Demographics
Physiologic anisocoria is usually less than 1.0 mm and can change from day to day.
It is as common in men as in women, in the morning as in the afternoon, in the young as in the aged. The prevalence of physiologic anisocoria is approximately 20%.
Significant History
History of optic nerve disease or retinopathy
Recent changes in pupil size
Ancillary Tests
Swinging flashlight test: In this test, light is directed first into one pupil, then moved over quickly to the other pupil, and repeated several times while both pupils’ response is observed. The test is done in a dimly lit room, with the patient gazing at a distant target and not at the light source. Allow just 3 to 5 seconds of illumination on each side.
When both afferent pathways are normal, the pupils remain essentially the same size no matter which side is illuminated. When an afferent defect is present, the pupils become larger when the light is directed to the involved side (see Fig. 19-1).
The RAPD can be measured subjectively or objectively with neutral density filters.
To measure an RAPD objectively, a neutral density filter is held in front of the uninvolved eye as the swinging flashlight test is performed. The filter density is increased until the pupil reactions on the swing test are equal.
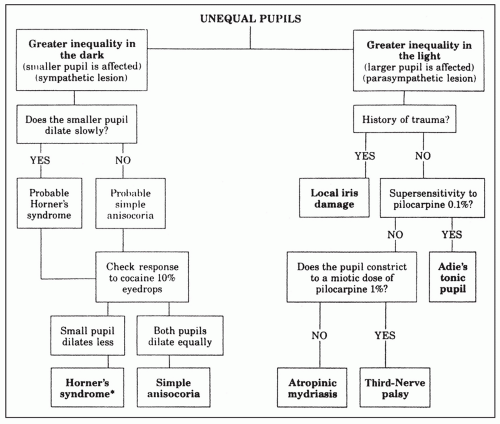 Figure 19-2. Flow chart for evaluation of anisocoria. (Reprinted from Multack RF, Lannin WC, Olbum JR. Improving diagnostic acumen in pupillary evaluation: a review for the primary care physician. J Am Osteopath Assoc 1989;89:917-924, with permission.) |
Anisocoria is evaluated by determining whether pupillary inequality is caused by a defect in sympathetic or parasympathetic innervation, or is because of a structural disorder of the iris. Therefore, a comparison of pupil size by measurement should be done in bright and dim ambient illuminations (Fig. 19-2).
The Treatment
The treatment of pupillary abnormalities is directed to the underlying cause. (See specific sections on optic neuropathies, retinopathy, Horner’s syndrome, Adie’s tonic pupil, Argyll Robertson pupil, third-nerve palsy).
Adie’s Tonic Pupil
Leonid Skorin Jr
Bruce G. Muchnick
ICD-9: 379.46
THE DISEASE
Pathophysiology
Tonic pupils occur from damage to the ciliary or the postganglionic short ciliary nerves that innervate the pupillary sphincter and ciliary muscles.
Selective damage causes areas of the iris to contract, with adjacent areas experiencing sector paralysis.
Etiology
Most cases of tonic pupil are idiopathic, although some follow a mild upper respiratory infection or other viral illness. Ocular and orbital trauma or surgery can also cause a tonic pupil.
If the tonic pupil is accompanied by diminished deep tendon reflexes, it is known as Holmes-Adie’s syndrome. This can be explained by concurrent involvement of the ciliary ganglion (tonic pupil) and dorsal root ganglion (areflexia).
Other causes of tonic pupil, especially if bilateral, include orthostatic hypotension, diabetes mellitus, Guillain-Barr’s syndrome, dysautonomias (such as Riley-Day’s syndrome), and acute ophthalmologic polyneuritis (Fisher’s syndrome). Other causes include infections, uveitis, sarcoidosis, orbital and intraorbital surgery, laser therapy, and trauma.
Bilateral tonic pupils that are mid-dilated and react poorly to light are also found in Parinaud’s dorsal midbrain syndrome. Unlike true Adie’s tonic pupils, these pupils constrict normally to convergence. Other signs of Parinaud’s syndrome include supranuclear paresis of vertical gaze, eyelid retraction, impaired vergence eye movements, convergence-retraction nystagmus, and skew deviation. These signs are not found in Adie’s tonic pupil.
The Patient
The patient is often asymptomatic or will have accommodative difficulties with anisocoria.
Clinical Symptoms
The patient with tonic pupil may complain of pupil size difference, photophobia, or blurred near vision with difficulty focusing.
Clinical Signs
Prominent Signs
Unilateral irregularly dilated pupil with poor to no response to light and shows a slow constriction to near stimulus with slow redilation
Subtle Signs
Sectoral iris paralysis
Irregular (vermiform) movements of the iris sphincter
Defective accommodation
Demographics
Up to 80% of tonic pupils are unilateral initially, and after 1 or 2 months, a tonic pupil may become miotic and smaller than the fellow pupil. Of the unilateral cases, approximately 4% become bilateral each year.
Tonic pupils occur in younger individuals (20 to 40 years of age), and there is a female predilection, with up to 70% of cases occurring in young women.
From 50% to 90% of patients with tonic pupil will also have diminished deep tendon reflexes.
Significant History
Recent viral illness
Ocular or orbital trauma
Hypotension
Diabetes
Ancillary Tests
Ocular assessment includes visual acuity, extraocular muscle testing, accommodation testing, slit-lamp evaluation of the iris, and fundus evaluation.
Pupil testing should be performed for light and near. To test for cholinergic supersensitivity, have the patient look at a distant target and administer pilocarpine 0.125% in each eye. Remeasure the pupil size after 15 minutes, making sure the patient does not do any near work.
The tonic pupil will constrict significantly as compared with the normal pupil.
Occasionally, an acute tonic pupil will not show cholinergic supersensitivity until several months later. No neuroimaging studies are necessary once the Adie’s tonic pupil is pharmacologically confirmed. All patients with bilateral tonic pupils, whether dilated or miotic, should have serological testing for syphilis FTA-ABS. Neurosyphilis may cause bilateral tonic pupil confirmed on cholinergic supersensitivity testing.
The Treatment
No treatment is necessary in an asymptomatic patient. If the patient is photophobic, dilute pilocarpine or tinted lenses can be helpful. Reading difficulties can be corrected with appropriate refractive correction for near work, often requiring unequal near adds. Consider colored contact lenses to hide any anisocoria.
Argyll Robertson Pupil
Leonid Skorin Jr
Bruce G. Muchnick
ICD-9: 379.45
THE DISEASE
Pathophysiology
The lesion responsible for pupillary abnormality is uncertain but may originate in the region of the Sylvian aqueduct in the rostral midbrain interfering with the light reflex fibers and supranuclear inhibitory fibers as they approach the Edinger-Westphal nuclei. The more ventrally located fibers for near response are not affected. In addition, the miosis found in classic Argyll Robertson’s syndrome can be explained by a lesion rostral to the oculomotor nuclei for pupillary constriction. This would interrupt the supranuclear inhibitory pathways from the higher brain centers thus producing a spastic paralysis in the oculomotor nuclei yielding a miotic pupil.
Etiology
The Argyll Robertson pupil has been recognized as the hallmark of late central nervous system (CNS) syphilis. Other possible causes include tabes diabetica, multiple sclerosis, encephalitis, sarcoidosis, chronic alcoholism, trauma, neoplasm, and diabetes mellitus.
The Patient
The patient will present with abnormal pupils characterized by miosis, unresponsiveness to light stimulus, and contraction on near effort in eyes with intact visual function.
Clinical Symptoms
The patient with Argyll Robertson pupils is often asymptomatic. The condition is typically bilateral and may be either symmetric or asymmetric. With few exceptions, it is permanent and usually stable but may deteriorate toward total pupil immobility. It develops over months to years.
If because of neurosyphilis, any signs that are present may include mixed neurologic features. These include meningeal syphilis (headache, nausea, vomiting, neck stiffness), microvascular syphilis (stroke), and parenchymal syphilis (paresthesias).
Clinical Signs
Prominent Signs
Miotic, irregular pupils that do not react to light but react briskly to a near stimulus
Subtle Signs
Pupils dilate poorly in the dark
Pupils dilate poorly to mydriatic agents
Usually bilateral but asymmetric
Iris atrophy
Demographics
Up to 80% of patients with neurosyphilis will have Argyll Robertson pupils.
Significant History
Tertiary syphilis
Diabetes mellitus
Demyelinating disease
Trauma
Neoplasm
Ancillary Tests
Ocular assessment includes visual acuity, extraocular muscle testing, testing pupillary reaction to light and near, slit-lamp evaluation for iris atrophy or interstitial keratitis, and fundus evaluation. Argyll Robertson pupils dilate poorly if the iris atrophy is extensive. The less the atrophy, the better the dilation. Likewise, miotics work poorly in the highly atrophied iris and well in the uninvolved iris. Iris atrophy may be visualized by transillumination of the globe.
Laboratory studies: VDRL, RPR, FTA-ABS, MHA-TP.
The Treatment
Treatment is indicated if there is active disease, and the patient should have an internal medicine evaluation.
Cat Scratch Disease
Joseph W. Sowka
Leonid Skorin Jr
ICD-9: 078.3
THE DISEASE
Pathophysiology
Cat scratch disease (CSD) is an infection caused by a fastidious Gram-negative bacillus from exposure to an infected cat or kitten. The most common manifestation of CSD in humans is regional lymphadenitis. Other systemic manifestations include Parinaud’s oculoglandular syndrome (conjunctivitis, retrotarsal conjunctival granulations, regional preauricular and cervical lymphadenitis, and fever), hepatosplenic infection, encephalopathy, osteomyelitis, and endocarditis. Fever, chills, abdominal pain, malaise and backache commonly occur. In immunocompetent individuals, the disease is typically self-limiting over the course of 3 to 6 weeks.
Beyond Parinaud’s oculoglandular syndrome, the ocular manifestation most associated with CSD is neuroretinitis, a combination of disc edema with stellate macular star of exudates. CSD appears to be the most common cause of neuroretinitis. In cases of neuroretinitis, vision is often affected, but to a variable degree. Vision may range from 20/20 to count fingers. Visual field defects are typically central and cecocentral scotomas. Dyschromatopsia and a relative afferent pupil defect may be present to variable degrees. Other posterior segment findings include peripapillary serous macular detachment, discrete foci of retinitis manifested as white retinal or choroidal lesions, vitritis, and submacular exudates. Anterior uveitis may also occur.
Etiology
The causative organism of CSD is the Gram-negative rod, Bartonella henselae. However, other strains of the organism, notably Bartonella quintana, have been implicated in the disease as well. The disease is transmitted by the scratch or bite of an infected cat or kitten, which are natural hosts for these organisms. About 10% of pet cats and 33% of feral cats are bacteremic with these organisms. Kittens are more likely than adult cats to carry the blood-borne bacteria and are the more common vector. Arthropod vectors exist as well, but transmission through fleas is questionable. Fleas are, however, the most likely transmission source between cats. The likely means of transmission of B. henselae from cats to humans may be inoculation with bacteria-containing flea feces through a contaminated cat scratch wound or across a mucosal surface. There may or may not be an identified history of a scratch or bite, but contact with felines is present. Ticks can also transmit this disease at the same time as Lyme’s disease. However, CSD is often overlooked in these cases of coinfection due to similar manifestations.
After an incubation period of several days to weeks, the patient develops a self-limiting regional lymphadenopathy with a small cutaneous lesion at the site of inoculation. The patient will demonstrate fever and flu-like symptoms, which will typically resolve over 3 to 6 weeks.
The Patient
The patient is typically younger and has had exposure to cats or kittens. Often there will be a history of a bite or scratch, but this history is not always present as
transmission across a mucosal surface is possible. The patient will manifest a flu-like illness with lymphadenopathy and fever.
transmission across a mucosal surface is possible. The patient will manifest a flu-like illness with lymphadenopathy and fever.
Clinical Symptoms
Regional lymphadenopathy
Fever
Malaise
Small cutaneous lesion at site of inoculation
Parinaud’s oculoglandular syndrome
Painless vision loss (typically unilateral)
May be asymptomatic
May diminish to count fingers
Dyschromatopsia
Clinical Signs
See Figure 19-3.
Conjunctivitis
Retrotarsal conjunctival granulations
Regional preauricular and cervical lymphadenitis
Stellate neuroretinitis (disc edema with macular star of exudates): Macular star may develop late in the disease
Vision ranging from 20/20 to count fingers
Relative afferent pupil defect (±)
Anterior uveitis
Focal retinochoroiditis
Submacular exudates with overlying serous retinal detachment
Disc edema
Disc edema with associated peripapillary or macular serous retinal detachment
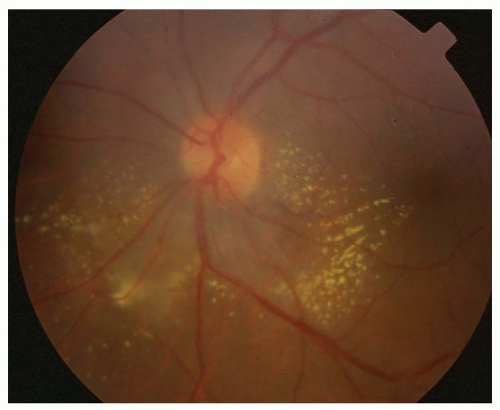 Figure 19-3. Cat scratch disease. |
Demographics
CSD typically afflicts young, otherwise healthy adults. It occurs commonly in children. Higher incidence is reported in fall and winter, attributed to seasonal breeding of cats.
Significant History
Despite the name, a scratch or bite from a cat is not always present. However, contact or exposure to cats or kittens is invariably reported. Patients may not remember a scratch or bite, but the disease is suspected in patients developing painless vision loss or disc edema following a febrile illness.
Ancillary Tests
The definitive test for CSD is the ELISA B. henselae titer. In that there are other species that can cause CSD, it is appropriate to obtain titers for B. quintana (and possibly Bartonella clarridgeiae) as well. Sera from 95% of patients with clinically defined CSD show IgG titers of 1:64 and above. Early in the disease process, IgG may be absent, but IgM may be positive. In some cases, there will be a false-negative ELISA despite clinical signs and symptoms of CSD. An alternate diagnostic modality is a polymerase chain reaction analysis of lymphadenopathy aspirate and should be considered in the clinical situation where CSD is strongly suspected and ELISA titers are either negative or borderline.
The Treatment
In immunocompetent individuals, CSD is generally a benign self-limiting disease with an excellent prognosis with little chance for morbidity. Without ocular involvement and visual loss, medical treatment is generally unnecessary.
The organism is quite susceptible to a number of antibiotics, such as penicillin, cephalosporins, aminoglycosides, tetracyclines, macrolides, fluoroquinolones, sulfamethoxazole, and trimethoprim, and rifampicin. Though antibiotics are frequently used for CSD neuroretinitis, there are no controlled clinical trials that indicate a better clinical outcome from this therapy. While the benefit of therapy in immunocompetent patients is unknown, cases complicated by ocular involvement are recommended for therapy. Azithromycin is the drug of choice if treatment is initiated. For pediatric patients, an initial dose of 10 mg/kg on the first day, followed by 5 g/kg/d for the following 4 days is the recommended regimen. For older children and adults, the recommended regimen is 500 mg on the first treatment day, followed by 250 mg/d for the next 4 days. This is most often used when there is vision loss from neuroretinitis. Whether oral prednisone has a role in the management of this disease is unknown.
Long-term prognosis for patients with ocular involvement is good, but some individuals may acquire a mild postinfectious optic neuropathy.
Horner’s Syndrome
Alan G. Kabat
Leonid Skorin Jr
ICD-9: 337.9—UNSPECIFIED DISORDER OF AUTONOMIC NERVOUS SYSTEM
ICD-9: 954.0—INJURY TO CERVICAL SYMPATHETIC NERVES
THE DISEASE
Pathophysiology
Partial or complete interruption of the oculosympathetic pathway results in Horner’s syndrome. The oculosympathetic pathway is composed of three neurons:
The first-order neuron arises from the posterior hypothalamus, traveling through the brainstem and cervical cord, and synapsing at the ciliospinal center of Budge at C8-T2.
Preganglionic second-order neuron fibers exit the spinal cord with the first ventral thoracic root and continue through the stellate ganglion at the pulmonary apex to the superior cervical ganglion at the bifurcation of the internal and external carotid arteries (C3-4).
The postganglionic third-order neuron originates from the superior cervical ganglion and travels along the internal carotid artery, penetrating the base of the skull and continuing through the cavernous sinus. The fibers that will innervate the eye and Müller’s muscles of the eyelids then enter the orbit via the superior orbital fissure. Fibers destined for the dilator muscle enter the eye via the long posterior ciliary nerves.
Etiology
First-order neuron lesions (50% to 60%)—Cerebrovascular disease (Wallenberg’s lateral medullary plate infarction syndrome), cervical trauma, Arnold-Chiari malformation, demyelinating disease (e.g., multiple sclerosis), syringomyelia, tumors of the pons, third ventricle, cervical cord or pituitary, osteoarthritis of the neck with bony spurs.
Second-order neuron lesions (20% to 30%)—Tumors of the chest apex (Pancoast’s tumor) or superior mediastinum, lymphadenopathy, aortic aneurysm, thyroid enlargement, surgical intervention (thyroidectomy, radical neck surgery, carotid angiography).
Third-order neuron lesions (20%)— Vascular headache syndromes (migraine, cluster, Raeder’s paratrigeminal neuralgia), cavernous sinus or middle cranial fossa lesions, basal skull fracture, carotid-cavernous
fistula, nasopharyngeal carcinoma, otitis media, sinusitis, trigeminal herpes zoster, Tolosa-Hunt’s syndrome, carotid artery occlusion or dissection.
Congenital—Birth trauma sustained during labor or delivery, cervical and mediastinal neuroblastoma.
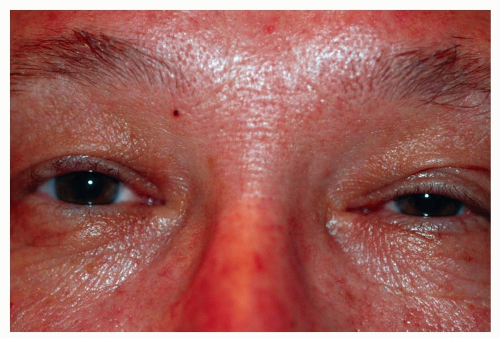 Figure 19-4. Horner’s syndrome. Ptosis, miosis on left side. |
The Patient
The classic Horner’s syndrome triad consists of unilateral ptosis, miosis, and anhidrosis (Fig. 19-4).
Clinical Symptoms
A patient with a recent onset of Horner’s syndrome will complain of a droopy eyelid and a lack of sweating on one side of the face, provided the lesion occurs distal to the carotid bifurcation, since most of the sudomotor sympathetic fibers to the face travel with the external carotid artery.
Clinical Signs
Prominent Signs
Anisocoria, which is greater in dim illumination
Upper eyelid ptosis
Diminished iris pigment in the affected eye (heterochromia iridis), if congenital
Subtle Signs
Upside-down ptosis or elevation of the lower eyelid
Apparent enophthalmos from a narrowed palpebral fissure
Dilated conjunctival and facial vessels
Decreased intraocular pressure
Increased accommodative amplitude
Absence of dilation to psychosensory stimuli
Demographics
Horner’s syndrome can occur in any patient regardless of gender or age. In those 20 years and younger, trauma is the most significant cause. From 21 to 50 years, almost half the cases result from tumors. In patients over 50 years of age, neoplasia is the most important cause. Horner’s syndrome is the initial sign of malignancy in 35% of patients. Overall, the cause of Horner’s syndrome can be identified in only about 60% of patients.
Significant History
New onset of headache
Trauma
Recent cardiac, neck, or thoracic surgery
Recent stroke
Ancillary Tests
Ocular assessment includes visual acuity, extraocular motility, levator function, pupil testing, visual fields, biomicroscopy, and fundus evaluation. Examination of old photographs may be helpful in determining the duration of the condition. Definitive diagnosis is based on pharmacologic pupillary testing to cocaine and hydroxyamphetamine.
Cocaine test. Cocaine produces dilation of the pupil by preventing reuptake of norepinephrine. If the sympathetic innervation to the eye is interrupted at any level (central, preganglionic, or postganglionic), cocaine will have no dilation effect. Cocaine helps confirm the presence or absence of oculosympathetic palsy by increasing pupillary
inequality; however, this test does NOT indicate the location of the lesion. (Note: patients may test positive on drug testing for 48 hours following the cocaine test.)
Cocaine (4% to 10%), one drop is placed in each eye and then repeated in several minutes. The pupils should be evaluated after 50 to 60 minutes. A Horner’s pupil does not dilate as well as the normal pupil.
Hydroxyamphetamine test. Hydroxyamphetamine (Paredrine) 1% causes a release of norepinephrine from the nerve endings at the myoneural junction, stimulating the dilator muscle. This helps distinguish a third-order neuron from a first-order neuron and second-order neuron. Third-order neuron lesions are considered to be “benign” while first- and second-order lesions are potentially life threatening.
Hydroxyamphetamine testing should not be performed for 48 hours following the cocaine test.
Hydroxyamphetamine 1% is placed in each eye, repeating one drop 1 minute later. The pupils are evaluated in 30 minutes. The normal pupil will dilate, while a third-order neuron lesion pupil will show no dilation. Pupillary dilation will be normal if the Horner’s syndrome is a result of a lesion to the first-order or second-order neuron.
Laboratory studies. Lab studies are not diagnostic of Horner’s syndrome, but may aid in identifying the underlying etiology. Complete blood count (CBC) with differential, syphilis testing (FTA-ABS and RPR), and purified protein derivative for tuberculosis should be considered. Imaging studies may include chest x-ray with lordotic view to image the lung apex, computed tomography (CT) scan, or magnetic resonance imaging (MRI) of the brain, and x-rays of the cervical spine.
If a central lesion is suspected, the patient should be referred for a neurology consult. Likewise, if malignancy is suspected, referral to an internist or oncologist is indicated. Vascular lesions warrant consultation with a vascular or thoracic surgeon.
The Treatment
Postganglionic lesions usually do not need treatment. Central or preganglionic lesions need to be addressed with appropriate consultation. Neurosurgical intervention may be required for potentially life-threatening situations. Vascular headache syndromes (e.g., migraine, cluster) should be treated to minimize recurrence.
Oculomotor Nerve Palsy
Joseph W. Sowka
Leonid Skorin Jr
ICD-9: 378.52
THE DISEASE
Pathophysiology
The oculomotor (third) cranial nerve innervates five extraocular muscles (the levator, superior, inferior and medial recti, and the inferior oblique) and carries the parasympathetic outflow to the ciliary ganglion, controlling pupillary constriction and accommodation. Any mechanism that disrupts this outflow will cause partial or complete oculomotor nerve palsy. Additionally, pupil dysfunction may also ensue.
Etiology
Causes of nuclear oculomotor nerve palsy include multiple sclerosis, vascular accidents, tumors, and infections. Midbrain vascular accidents account for the majority of fascicular palsies, involving both the oculomotor nucleus as well as the nerve’s fascicles as they course through the parenchyma of the midbrain. After exiting the brainstem
in the interpeduncular fossa, the oculomotor nerve passes inferolateral to the posterior communicating artery (PCA) and medial to the edge of the tentorium. In this region, it is vulnerable to damage from transtentorial herniation also known as uncal syndrome. Compression from an aneurysm of the PCA can also cause pupil-involving oculomotor palsy. Nerve damage can also result from subarachnoid hemorrhage and meningitis.
in the interpeduncular fossa, the oculomotor nerve passes inferolateral to the posterior communicating artery (PCA) and medial to the edge of the tentorium. In this region, it is vulnerable to damage from transtentorial herniation also known as uncal syndrome. Compression from an aneurysm of the PCA can also cause pupil-involving oculomotor palsy. Nerve damage can also result from subarachnoid hemorrhage and meningitis.
The disease processes within the cavernous sinus usually involve more than one nerve and include neoplasm, aneurysm, thrombosis, fistula, inflammation, and ischemia.
The oculomotor nerve divides into superior and inferior divisions at the level of the anterior cavernous sinus or superior orbital fissure. Superior-division palsies, involving the superior rectus and levator, may result from aneurysm, viral infection, diabetes, and enlargement of the third ventricle. Inferior-division palsies, involving the inferior rectus, inferior oblique, medial rectus, and ciliary sphincter, result from trauma, viral infections, local orbital disease, and brainstem vascular malformations. Orbital involvement, such as trauma, tumor, aneurysm, and infection from a tooth abscess, can damage the oculomotor nerve.
Aberrant regeneration or oculomotor synkinesis occurs only with mechanical disruption of fibers following an acute palsy such as from trauma or aneurysmal rupture and never from vasculopathic palsies. This type of misdirection can also be found in congenital oculomotor nerve palsy and ophthalmoplegic migraine. Patients with ophthalmoplegic migraine are children and young adults who have a strong family history of migraine.
The Patient
Symptoms and signs depend on the location of the lesion that is disrupting the oculomotor nerve. Identifying pupil involvement is critical to diagnosis and management.
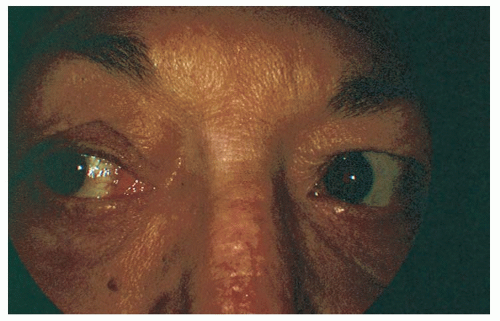 Figure 19-5. Oculomotor nerve palsy. Adduction deficit in partial oculomotor palsy. |
Clinical Symptoms
The patient with oculomotor nerve palsy will complain of diplopia, droopy eyelid, difficulty focusing or reading, and possible eye or hemicranial pain (Fig. 19-5).
Clinical Signs
Prominent Signs
Complete palsy, which includes ptosis and restriction of ocular movement except for abduction and intorsion. The pupil may also be fixed and dilated.
Superior-division palsy includes ptosis with a restriction in upgaze.
Inferior-division palsy includes restriction in downgaze, restricted adduction, and pupil dilation.
Nuclear-fascicular palsies may also involve contralateral hemiplegia, intention tremor, and ataxic gait depending upon the location of the damage within the midbrain.
Subtle Signs
Aberrant regeneration or oculomotor synkinesis
Loss of accommodation
Loss of near-light reflex
Demographics
Approximately 20% of oculomotor third-nerve palsies are a result of expansion or hemorrhage of an aneurysm,
and vasculopathic causes, such as diabetes, account for another 20%. Patients who have an underlying vasculopathic etiology are usually older than 45 years of age, and 60% or more are diabetic. Only 15% of oculomotor palsies are because of neoplasm. In children, 40% of oculomotor palsies are congenital, and 20% are because of trauma.
and vasculopathic causes, such as diabetes, account for another 20%. Patients who have an underlying vasculopathic etiology are usually older than 45 years of age, and 60% or more are diabetic. Only 15% of oculomotor palsies are because of neoplasm. In children, 40% of oculomotor palsies are congenital, and 20% are because of trauma.
The pupil is spared in 80% of vasculopathic oculomotor nerve palsies and involved in 95% of aneurysmal palsies. Patients developing oculomotor nerve palsy from aneurysmal compression may initially not present with anisocoria or pupil involvement but may evolve and develop pupil dilation over several days. Lesions in the cavernous sinus also may spare the pupil or present with a concurrent Horner’s syndrome. Approximately one third of patients with CN III palsy from vascular infarct manifest a small degree of anisocoria of typically less than 1 mm. In contradistinction, aneurysmal compression typically causes more than 2 mm of anisocoria.
Significant History
Diabetes
Hypertension
Hyperlipidemia
Herpes zoster
Leukemia
New onset headache
Ancillary Tests
Ocular assessment includes visual acuity, extraocular muscle testing, visual field, exophthalmometry, levator function, and pupil assessment.
When the pupil is not involved, an edrophonium test, anticholinesterase antibody assay, evaluation of orbicularis strength, and evaluation of ptosis after sustained upgaze should be performed to rule out myasthenia gravis (MG) mimicking oculomotor palsy.
Neuroimaging with a CT or MRI and magnetic resonance angiography (MRA), lumbar puncture, or cerebral angiography is indicated for all pupilinvolved oculomotor palsies or pupilsparing palsies if the patient is less than 45 years old with no vasculopathic history, has incomplete palsy, has a palsy that has not shown any improvement over 3 months time, or has more than just an isolated oculomotor deficit. Any patient who develops aberrant regeneration should also have neuroimaging.
Laboratory studies: CBC with differential, glucose tolerance test, erythrocyte sedimentation rate (ESR), RPR, antinuclear antibody. A blood pressure measurement should also be done.
The Treatment
Most patients with ischemic oculomotor nerve palsies show improvement within 1 to 2 months and maximally by 6 months. In ischemic vascular CN III palsy, the pupil will not evolve and aberrant regeneration will not occur. While waiting for improvement to occur, the underlying vasculopathic abnormality should be corrected, and the patient may wear a temporary eye patch for any disturbing diplopic symptoms. Patients who have pupil-involving oculomotor palsies will need emergent evaluation and testing with possible hospitalization. If an intracranial aneurysm is the suspected cause of the oculomotor palsy, then the patient should be sent emergently to the hospital, as 20% of these patients die within 48 hours because of aneurysm rupture and subsequent subarachnoid hemorrhage. Close pupil observation is required as pupil involvement may be delayed by 5 to 7 days. This is especially true for patients with incomplete oculomotor nerve palsy as they are more likely to have an insipient aneurysm developing. Complete and total oculomotor palsy in an adult over age 50 without
pupil involvement is rarely ever caused by an aneurysm.
pupil involvement is rarely ever caused by an aneurysm.
Children with chronic oculomotor palsies may need Fresnel prism correction or botulinum toxin injection to the lateral rectus to prevent contracture of the muscle. Surgery should be delayed until 6 months from the time improvement has ceased. Ipsilateral horizontal recess-resect procedures work well if there is at least 50% medial rectus function. If the palsy is complete, large horizontal recess-resect procedures are combined with contralateral lateral rectus weakening and/or ipsilateral superior oblique transposition. Contralateral vertical muscle surgery may also need to be performed.
Trochlear Nerve Palsy
Joseph W. Sowka
Leonid Skorin Jr
ICD-9: 378.53
THE DISEASE
Pathophysiology
The trochlear (fourth) cranial nerve is the only cranial nerve that exits at the dorsal aspect of the brainstem. The nerve fibers then cross and follow a long and circuitous course from the brainstem to the superior oblique muscles. This makes the nerve vulnerable to injury at many locations.
Etiology
Causes of nuclear-fascicular trochlear nerve palsy include ischemia from infarction, hemorrhage, demyelination, compression, and trauma. Bilateral trochlear nerve palsies are often seen following blows to the head. Bilateral, and occasionally unilateral, trochlear nerve palsies can be associated with a tumor of the pineal gland compressing the posterior midbrain in the dorsal midbrain syndrome. Loss of upward saccades and a light-near dissociated pupil accompany the trochlear palsy in dorsal midbrain syndrome. Distention of the fourth ventricle or contrecoup forces transmitted to the brainstem by the free tentorial edge may injure the nerves. As the nerve courses through the cavernous sinus and orbit, it can be affected by inflammation, tumor, aneurysm, fistula, or trauma. Isolated trochlear nerve palsies may be congenital and appear in late childhood to mid-adult life as a result of decompensation. Otherwise, most isolated acquired trochlear nerve palsies are due to trauma, hypertension, atherosclerosis, and diabetes. More rare causes of palsy include herpes zoster ophthalmicus, collagen vascular disease, aneurysm, hydrocephalus, multiple sclerosis, polycythema vera, cat-scratch disease, and encephalitis.
The Patient
Most patients with trochlear nerve palsy will complain of vertical diplopia that is eliminated when one eye is closed (Fig. 19-6). Often, head tilting to the opposite side will relieve the diplopia or make the patient feel more comfortable.
Clinical Symptoms
Vertical diplopia that is worse in the field of action of the involved superior oblique muscle
Difficulty with near tasks or downgaze
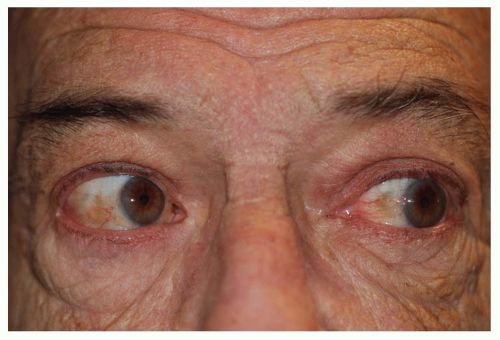 Figure 19-6. Trochlear nerve palsy. Right fourth nerve palsy. Right overaction on left gaze. |
Clinical Signs
Prominent Signs
Positive Parks “three-step test”
Step 1: Vertical deviation on the side of the lesion
Step 2: Vertical deviation worsens on gaze away from the involved nerve
Step 3: On Bielschowsky head-tilt testing, the deviation is greater on head tilt toward the involved trochlear nerve
Subtle Signs
Assumed or habitual head tilt toward the contralateral shoulder
Large vertical fusional amplitudes
Excyclotorsion as measured by double Maddox rod test
Hyperdeviation greater on downgaze
Demographics
The most common cause of trochlear nerve palsy is trauma, which constitutes approximately 40% of the cases. In spite of the availability of improved diagnostic techniques, the number of cases remaining without a specific diagnosis is still approximately 30%. Ischemia causes 20% and tumors and other sinister causes constitute 10% of acquired, isolated trochlear palsies.
Congenital trochlear palsies are also very common and can present in later life due to decompensation. Approximately 30% of all trochlear palsies are bilateral, and the prevalence increases to 40% in those secondary to trauma.
Significant History
Head trauma, especially blows to the vertex
Hypertension
Diabetes
Ancillary Tests
Ocular assessment includes visual acuity, extraocular muscle testing including the Parks three-step test and Bielschowsky’s head-tilt testing. Measurement for excyclotorsion can be done with a double Maddox rod in a trial frame or phoropter, Maddox wing, or Lancaster red/green test. Cyclotorsion can also be evaluated with fundus examination or photography. Normally, the optic nerve is just slightly higher than the foveal area. In trochlear nerve palsy, the optic disc is significantly higher than the fovea on fundus photography and lower on indirect ophthalmoscopy.
If congenital trochlear nerve palsy is suspected, then measurement of the amplitude of vertical vergence should be done. In most patients, the normal value of vertical fusional amplitude is from 3 to 6 prism diopters. Patients with congenital trochlear palsy may be able to fuse anywhere from 10 to 30 prism diopters of deviation (using vertical prism bars). Evaluate possible long-standing palsy by reviewing old photographs, looking for the presence of head-tilting. Further, immediately upon entering the examination room, unobtrusively look for the presence or absence of a head-tilt.
Laboratory studies: Glucose tolerance test, ESR, C-reactive protein (CRP), blood pressure measurement, edrophonium test, and/or anticholinesterase antibody assay if MG is suspected.
If the palsy has not resolved or improved in 4 months, or if any other neurologic signs are present, then the patient will also need neuroimaging, lumbar puncture, and cerebral angiography. If the patient has developed trochlear nerve palsy from recent head trauma, the patient should undergo neuroradiological studies of the head to dismiss the possibility of a concurrent subarachnoid hemorrhage. In patients under age 40 with a sudden onset of trochlear nerve palsy, no ischemic vascular diseases such as diabetes and hypertension, and there is no evidence that the diplopia is a result of decompensation of a longstanding condition, then neuroimaging is indicated.
The Treatment
Because many acquired trochlear nerve palsies spontaneously recover in 4 to 6 months, observation with patching for symptomatic diplopia is sufficient. If the deviation remains stable, prisms incorporated into glasses may be of benefit. Surgical correction has a high success rate. Surgery is undertaken when the deviation has been stable for at least 6 months. Botulinum injections may be considered as well.
Abducens Nerve Palsy
Joseph W. Sowka
Leonid Skorin Jr
ICD-9: 378.54
THE DISEASE
Pathophysiology
The abducens (sixth) cranial nerve originates in the dorsal midpons with its nucleus being surrounded by the seventh-nerve fascicle. This complex anatomic relationship helps determine the presence of associated findings. The abducens nerve fascicle travels anteriorly through the pons, lateral to the parapontine reticular formation, and through the pyramidal tract to exit the brainstem into the subarachnoid space. Due to the close anatomic relationships between these structures, isolated abducens palsy due to damage within the midpons is unlikely. The subarachnoid space is the most common locus of isolated, unilateral abducens nerve palsy. The abducens nerve then continues up the clivus, over the petrous ridge along the base of the skull, entering the cavernous sinus and the orbit to innervate the lateral rectus muscle.
Etiology
Causes of nuclear-fascicular abducens nerve palsies include tumors, demyelination, and vascular disease. The abducens nerve is vulnerable in the subarachnoid space from trauma and tumors. It is here that the nerve is affected by elevated intracranial pressure by downward displacement of the brainstem and secondary stretching of the nerve. This will manifest often as a bilateral abducens palsy with concurrent papilledema. Inflammation of the petrous bone and its dura may occur secondary to middle-ear infections, known as Gradenigo’s syndrome. Traumatic abducens nerve palsies may result from basilar skull fractures. Masses invading the base of the skull from the nasopharynx or at the cerebellopontine angle may cause abducens-nerve pareses.
Cavernous sinus and orbital etiologies include trauma, diabetes, hypertension, tumor, aneurysm, fistula, inflammation, and cellulitis. Isolated abducens nerve palsy is seen in young patients with postviral syndrome and in adults with hypertension or diabetes with ischemic mononeuropathy.
The Patient
Most patients with isolated abducens nerve palsy will complain of horizontal diplopia, which is greater at distance and is eliminated when one eye is closed. There are three distinct patient groups experiencing abducens palsy: children, young adults, and older adults.
Clinical Symptoms
Horizontal diplopia, worse at distance than near and exaggerated when the patient looks in the direction of the affected lateral rectus muscle.
Clinical Signs
Prominent Signs
Abduction deficit
Esotropia greater with paretic eye fixing a distant target, compared with unaffected eye fixing target
No restriction on forced duction testing
Associated Syndromes
Millard-Gubler—Ipsilateral abducens, and facial-cranial nerve palsy with contralateral hemiparesis
Raymond-Cestan—Ipsilateral abducens palsy with contralateral hemiparesis
Foville’s—Ipsilateral gaze palsy; ipsilateral trigeminal and facial-cranial nerve palsy with ipsilateral Horner’s syndrome
Gradenigo’s—Ipsilateral trigeminal pain, abducens, facial-cranial nerve palsy, and hearing loss
Pseudo-Gradenigo’s—Ipsilateral abducens palsy, ipsilateral trigeminal pain, ipsilateral ocular irritation, and hearing loss
Demographics
Abducens nerve palsies occur more frequently than do palsies of the oculomotor or trochlear cranial nerve. Up to 30% of the time, the exact cause of abducens palsy remains unknown, while the rest of the time there appears to be an even distribution between tumor, vasculopathic causes, and trauma. Bilateral abducens nerve palsies rarely result from vascular disease and are more common in children than in adults. Bilateral abducens palsies, especially with concurrent optic disc edema, strongly suggest increased intracranial pressure.
Significant History
Head trauma
Diabetes
Hypertension
New onset of headache, tinnitus, transient visual obscurations, nausea if increased intracranial pressure is suspected
Possible associated hemi-paresis, facial nerve paralysis, Horner’s syndrome, otitis media
Ancillary Tests
Ocular assessment includes visual acuity, extraocular muscle testing, forced duction testing, corneal sensitivity with cotton wisp, orbicularis strength, slit-lamp exam, and funduscopic evaluation for papilledema.
Laboratory studies: CBC with differential, glucose tolerance test, ESR, CRP, RPR, antinuclear antibody, and blood pressure measurement.
Neuroimaging with MRI if a lesion of the brainstem or posterior fossa is suspected. CT scanning is preferred if sinus or mastoid disease is suspected. Lumbar puncture and cerebral angiography may also be necessary.
Edrophonium testing and/or acetylcholinesterase antibody assay is indicated if myasthenia is a concern.
In children, nearly half of all abducens palsies are due to a CNS lesion. Neurologic evaluation, neuroimaging, and consultation is urgent in this group and the cause of the palsy shouldn’t be presumed to be benign.
In younger adults, CN VI palsy is likely to be caused by CNS mass lesions and multiple sclerosis. Thus, neuroimaging is highly recommended in this group.
There is a very low risk of acute isolated abducens palsy in an older adult being cause by an aneurysm, neoplasm, or demyelization. Isolated abducens palsy in older adults with a history of diabetes or hypertension do not need neuroimaging or other extensive evaluation unless the palsy progresses, fails to improve over 3 months, or other neurologic complications develop.
The Treatment
In an acute phase of an abducens cranial nerve palsy, simple occlusion with patching or temporary prisms if the deviation is small and not greatly noncomitant may be all that is necessary. Botulinum toxin injections into the ipsilateral medial rectus muscle may be necessary if the recovery is prolonged or the deviation is too
large for prism correction or to prevent secondary contracture of the medial rectus. Surgical correction can be done after measurements have been stable for at least 6 months. An ipsilateral recess-resect procedure combined with a contralateral medial rectus recession may be indicated.
large for prism correction or to prevent secondary contracture of the medial rectus. Surgical correction can be done after measurements have been stable for at least 6 months. An ipsilateral recess-resect procedure combined with a contralateral medial rectus recession may be indicated.
Any underlying identified medical problem must be addressed.
Facial Nerve Palsy
Leonid Skorin Jr
ICD-9: 351.0
THE DISEASE
Pathophysiology
Facial palsy is the most common of the cranial neuropathies. Bell’s palsy is a facial palsy of no obvious cause whose presumed mechanism is swelling of the peripheral portion of the facial or seventh cranial nerve because of immune or infectious disease. The nerve becomes compressed and ischemic in its narrow course through the temporal bone. This mechanical compression causes interruption of the nerve’s transmission, resulting in a conduction block and nerve degeneration. Additional immunological response may result in fragmentation and demyelination of the nerve sheath, causing loss of function. Because this condition is temporary, remyelination occurs after the inflammation resolves.
Etiology
True Bell’s palsy or idiopathic facial palsy has no known underlying cause. Recent findings now strongly point to herpes simplex virus type I as the most likely cause of Bell’s palsy. Other viral infections such as varicella-zoster, Epstein-Barr (infectious mononucleosis), measles, rubella, rabies, mumps, cytomegalovirus, infectious hepatitis, and human immunodeficiency are also known to cause facial palsy.
Herpes zoster can cause up to 13% of facial palsies. Herpes zoster infection of the geniculate ganglion with typical herpetic vesicular eruptions is known as Ramsay Hunt’s syndrome (herpes zoster oticus).
Bacterial infection is the cause of facial palsy up to 4% of the time. Tetanus, brucellosis, typhoid fever, leptospirosis, and diphtheria are rare examples. In endemic areas, up to 25% of acute facial palsies may be caused by Lyme’s disease. Lyme’s disease is a systemic spirochetal infection with Borrelia burgdorferi that follows the bite of the deer tick.
Facial palsy can be the result of middle-ear disease (otitis media with or without mastoiditis); malignancies of the parotid gland because the facial nerve runs through the gland; and neoplasms, both primary, such as schwannomas, or secondary, such as acoustic neuromas, which cause compression at the cerebellopontine angle. Up to 21% of the time, trauma is the cause. Primary neurologic disorders, such as Guillain-Barré and Melkersson’s syndrome, may also cause facial palsy.
The Patient
Symptoms and signs may range from subtle weakness and facial muscle paresis to complete unilateral paralysis.
Clinical Symptoms
The patient with Bell’s palsy complains of sudden unilateral facial weakness. There may be drooling after brushing the teeth or when drinking, an asymmetric appearance of the mouth, an inability to whistle, and excessive epiphora. The patient may describe deadness, loss of feeling, or numbness. Up to 50% of patients experience pain behind the ear, sometimes even preceding physical changes. Hyperacusis (painful response
to sound) and dysgeusia (distorted taste) are also common.
to sound) and dysgeusia (distorted taste) are also common.
Clinical Signs
Prominent Signs
Complete unilateral facial paresis or paralysis involving the forehead, orbicularis oculi, facial muscles of expression, and mouth (Figs. 19-7 and 19-8).
Subtle Signs
Loss of facial creases and folds
Widening of the palpebral aperture
Lower lid ectropion
Inability to blink
Down turning of one side of mouth
Corneal irritation from dry eye and exposure
Demographics
Bell’s palsy is the most common peripheral facial palsy, occurring in 20 per 100,000 to 40 per 100,000 persons annually. Men and women of all ages are equally affected, with the majority of patients between the ages of 20 and 40. The condition affects the left and right sides of the face with equal frequency. It is bilateral at onset in about 0.3% of cases and recurrent in up to 11%. Up to 31 % of patients with recurrent Bell’s palsy are diabetics. A family history can be obtained in 2% of patients. The disease is 3.3 times more common in pregnant women and is especially prevalent in the third trimester or within the first week postpartum.
 Figure 19-7. Facial nerve palsy. Bell’s palsy, right side. Inability to close right eyelid. |
 Figure 19-8. Facial nerve palsy. Bell’s palsy, right side. Inability to furrow right frontalis muscles. |
Significant History
Prior exposure to stress, upper respiratory infection, cold, fever, dental extraction, menstruation, or driving with cold air blowing on the face
Pregnancy
Diabetes
Hypertension
Exposure to tick bite and skin rash (erythema chronicum migrans)
Medical history of Guillain-Barré, Lyme’s disease, sarcoidosis, carcinomatous, treponemal, mycobacterial or cryptococcal meningitis, multiple sclerosis, if bilateral palsy is present
Ancillary Tests
Ocular assessment includes visual acuity, extraocular muscle testing, noting any muscle imbalance or nystagmus, corneal sensitivity with cotton wisp, slit-lamp exam with fluorescein, and rose bengal staining, Shirmer basal secretion test, orbicularis strength, and Bell’s phenomenon. Otologic evaluation of the ear canal and tympanic membrane, looking behind the ear, hearing test in suspected cases of Ramsay Hunt’s syndrome.
Ancillary studies include CBC with differential, urinalysis, plasma glucose, ESR, chest x-ray, and Lyme titer. In patients with complete paralysis, assessment of neural status by electrical tests is useful. These include maximal
nerve stimulation, nerve conduction, electromyography (EMG), and electroneuronography (ENOG). Imaging studies (MRI, CT) are indicated when the history or physical examination turns up suspicious findings or when facial movement does not recover within 6 months.
nerve stimulation, nerve conduction, electromyography (EMG), and electroneuronography (ENOG). Imaging studies (MRI, CT) are indicated when the history or physical examination turns up suspicious findings or when facial movement does not recover within 6 months.
The Treatment
The one essential intervention in any facial palsy is corneal protection. Nonpreserved artificial tears during the day and bland ointment at night are mandatory. The patient may also physically close his or her eyelids when the eye is irritated. Moisture chambers, eyelid taping, external eyelid prosthesis, punctal plugs, botulinum toxin injection to induce upper eyelid ptosis, surgical placement of a stainless steel spring or gold weight to reanimate the upper eyelid, or partial tarsorrhaphy should be considered in cases of corneal compromise.
If the patient is seen within 2 weeks of onset of symptoms, oral prednisone 1 mg/kg of body weight daily (60 mg/d maximum) for 7 days, split into twice-daily dosing, then tapered over a subsequent 3 days can be started. Oral prednisone is most beneficial in patients with pain and complete paralysis. If seen within the first 3 days of symptom onset, oral antiviral agents (acyclovir 400 mg five times daily for 10 days, valacyclovir 500 mg three times daily for 7 days, or famciclovir 500 mg three times daily for 7 days) may be added to suspected herpes simplex palsies. The Quality Standards Subcommittee of the American Academy of Neurology recommends that the use of steroids is probably effective and under most circumstances should be considered but that antiviral agents should only possibly be considered.
Oral antiviral agents should be used in all cases of Ramsay Hunt’s syndrome. Lyme facial palsy is treated with amoxicillin, 500 mg four times a day for 3 to 4 weeks, or doxycycline, 100 mg two or three times a day for 3 to 4 weeks. Ceftriaxone, a third-generation cephalosporin, is used in amoxicillin and doxycycline failures.
Middle cranial fossa surgical decompression is of benefit in cases of complete acute paralysis between 3 and 14 days after onset, ENOG with more than 90% degeneration, and voluntary EMG with no motor-unit potentials.
Cerebral Venous Thrombosis
Bruce G. Muchnick
ICD-9: 325
THE DISEASE
Pathophysiology
Cerebral venous thrombosis (CVT) describes the presence of a blood clot, or thrombus, within the venous system of the brain. This may lead to partial or complete occlusion of a cerebral vein, resulting in neurologic and visual dysfunction. The blocking of a cerebral vein or dural sinus causes blood to be forced retrograde into the capillaries. This blocks oxygenated blood to the cerebral tissues, leading to ischemia, edema, and hemorrhagic infarction.
Etiology
A thrombus is an insoluble mass formed in the vascular system and composed of constituents of the blood. It forms on and is attached to the endothelium of the blood vessel. It may partially or completely occlude the lumen of the vessel.
The thrombus is composed primarily of platelets and fibrin. There may be an inflammatory response in the vessel wall accompanying the blood clot.
CVT is caused by infectious or noninfectious processes. Acute inflammation
can reach the cerebral veins and arise from infections of the mastoid air cells and paranasal sinuses. Infectious sources include fungi, virus (HIV), parasites (trichinosis), and bacteria (syphilis).
can reach the cerebral veins and arise from infections of the mastoid air cells and paranasal sinuses. Infectious sources include fungi, virus (HIV), parasites (trichinosis), and bacteria (syphilis).
Aseptic occlusion of the intracerebral venous structures can be caused by trauma, tumors, systemic diseases (lupus and Behçet’s disease), hypoperfusion (heart failure), and most commonly hypercoagulability.
No matter what the cause, cerebral venous occlusion results in hemorrhagic infarction of brain tissue and cerebral and subarachnoid hemorrhage.
Cerebral sinovenous thrombosis may be caused by closed head injury, with the stroke occurring usually within 4 days of the injury. Other causes include the use of oral contraceptives and pregnancy, but in 30% of cases, no etiology is discovered.
Dietary fasting has been shown to increase the frequency of CVT. Other risk factors include the human immunodeficiency virus (HIV), developmental venous anomalies, inflammatory bowel disease, and inner ear infection.
The Patient
Clinical Symptoms
A low grade venous sinus thrombosis may be so mild as to produce only an increase in intracranial venous pressure, resulting in a mild headache. However, the most common presenting complaint in adults is severe headache. Focal seizures may occur if there is partial ischemia to the cerebral cortex. These seizures are sometimes preceded by a prodrome of numbness, weakness, behavioral changes, and headache. A variety of visual field defects, either permanent or transient, may result from venous sinus thrombosis.
Clinical Signs
Depending on the location of the thrombosis, a wide range of neurological deficits may accompany cerebral venous thrombosis, including aphasia, memory loss, chills, sweats, and tachycardia. Ocular manifestations include pain around the eyes, orbital congestion, lid swelling, proptosis, and ophthalmoplegia.
An increase in cerebral spinal fluid level may result in papilledema.
The most common presenting signs and symptoms in children with CVT include headache, vomiting, visual disturbance, papilledema, fever, and sixth-nerve palsy. Half of all children (age 1 month to 17 years) had adverse outcomes following treatment, including chronic intracranial hypertension, residual hemiparesis, permanent sixth-nerve palsy, and death.
Cerebral venous thrombosis is more common in women, who develop the condition younger than men and more commonly have the symptom of headache upon presentation. One possible explanation is that 65% of women have a gender-specific risk factor, such as oral contraceptives, pregnancy, or hormonal replacement.
Demographics
Overall, CVT occurs in three to four cases per million people per year worldwide; in children, the incidence doubles to seven cases per million. Because of the introduction of antibiotics, septic thrombosis has become relatively rare and accounts for about 10% of all cases of cerebral venous thrombosis in the Western world. In developing countries, the rate is higher (25%). The most common cause of aseptic venous thrombosis is hypercoagulability, most commonly from the use of oral contraceptives. One study showed that in cases of cerebral venous thrombosis, 12% were deceased within 3 years, 12% had seizures, 10% had motor deficits, 8% had visual field defects, 45% had headaches, and 83% were living independent lifestyles.
Significant History
Inquire about the sudden onset of neurological deficits.
Is the patient taking medications that may contribute to hypercoagulability states (birth control pills)?
Is there any genetic disorder in the family or patient that may lead to a hypercoagulability state?
Has there been any blunt injury to the head?
Did the patient receive electroconvulsive treatment?
Does the patient have any known systemic disorders?
Does the patient have any signs of infection of the head or neck?
Ancillary Tests
The primary method of diagnosing cerebral venous thrombosis is noninvasive neuroimaging. This includes CT scanning and MRI. CT scanning may be performed unenhanced or with injection of iodinated contrast material. T1- and T2-weighted MR images in patients with venous thrombosis reveal abnormalities in the veins and sinuses.
MR angiography (3D MR flow imaging) can reveal abnormalities in the intracranial and extracranial vasculature. Conventional (invasive) angiography can then confirm the diagnosis of thrombosis.
Laboratory tests (CBC with differential, blood cultures) should be utilized to rule out sepsis.
Blood tests are helpful to detect a hypercoagulability state. These include CBC, ESR, CRP, prothrombin time, partial thromboplastin time, protein S deficiency, protein C deficiency, antithrombin III, factor V Leiden (activated protein C resistance), anticardiolipin profile, lupus anticoagulant, and homocysteine.
The Treatment
Treatment depends on the underlying cause of the thrombosis and location and severity of the neurological deficit.
Septic thrombosis requires antimicrobial treatment and possible surgery
Blood thinners (Heparin) are used in many cases to treat aseptic thrombosis
Urokinase (thrombolysis) can be used in aseptic thrombosis
Surgical removal of the thrombus: Decompressive hemicraniectomy improves morbidity and mortality in severe CVT
Stent placement
Treatment of elevated ICP (acetazolamide), lumbar punctures, or shunt procedures
Long-term blood-thinner therapy (Warfarin)
Men have an average of 71 % complete recovery
Women have a better prognosis than men (81% exhibit complete recovery).
After 5 years, patients report long-term problems including impaired concentration (75%), headache (43%), depression (30%), and fatigue (30%); and 20% were unemployable.
Thirteen percent of patients have a poor clinical outcome.
Cavernous Sinus Syndrome
Leonid Skorin Jr
Bruce G. Muchnick
ICD-9: 437.6—NONPYOGENIC THROMBOSIS OF INTRACRANIAL VENOUS SINUS
ICD-9: 325—PHLEBITIS AND THROMBOPHLEBITIS OF INTRACRANIAL VENOUS SINUS



