Neck masses often present physicians with a challenging exercise in differential diagnosis. These masses occur among all age groups and may have a wide variety of causes, including congenital, inflammatory, neoplastic, and other conditions (Table 33-1). This chapter focuses on the basic evaluation of a neck mass and provides an overview of some of the more common neck masses.
MEDICAL HISTORY AND PHYSICAL EXAMINATION
A thorough medical history and physical examination are crucial in evaluating a neck mass. Narrowing the differential diagnosis facilitates selection of appropriate ancillary tests. The history must include the age of the patient, the duration and rate of growth of the mass, other local and regional symptoms, a social history, and the presence or absence of systemic symptoms.
Asymptomatic neck masses among adults older than 40 years should be considered malignant until proved otherwise. Eighty percent of nonthyroid and nonsalivary gland masses are neoplastic, and 80% of neoplastic masses are malignant. Among children, however, as many as 90% of neck masses are benign. Masses that grow slowly tend to be benign. A mass that appears suddenly or enlarges rapidly may be inflammatory or neoplastic.
All patients should be questioned regarding social habits (smoking, alcohol, or drug use) that may place them at a higher risk for head and neck tumors. Information must be obtained regarding human immunodeficiency virus status or risk factors, living environment, occupation, travel history, and family history of cancer. Neck masses accompanied by fevers, chills, night sweats, or myalgia may represent local manifestations of systemic disease, such as a lymphoproliferative or an inflammatory disorder. History regarding regional symptoms such as dysphagia, odynophagia, hoarseness, otalgia, and dyspnea should be obtained. A complete chest and abdominal examination should be performed to look for primary lesions in these areas. For adults, breast and rectal examinations must be performed, especially if neoplasia is suspected. Primary adenocarcinoma below the clavicles can spread to and present as cervical lymph nodes.
A complete otolaryngologic examination must be performed and include visualization of all mucosal surfaces of the nose, oral cavity, nasopharynx, oropharynx, hypopharynx, and larynx. The tongue base and oral cavity must be palpated. Flexible nasopharyngolaryngoscopy should be performed if mirror exam of the larynx is difficult or inadequate. Examination of the skin of the scalp, rest of the head, and neck helps rule out cutaneous lesions, such as melanoma, squamous cell carcinoma, or Kaposi’s sarcoma, as the cause of a neck mass. The neck must be carefully examined with specific regard to the points outlined below.
TABLE 33-1. Differential diagnosis of neck masses
Congenital
Branchial cyst
Lymphatic malformation
Thyroglossal cyst
Hemangioma
Teratoma
Dermoid cyst
Thymic cyst or mass
Laryngocele
Fibromatosis colli
Inflammatory
Cervical adenitis: bacterial (nonspecific or related to infection of tonsil or pharynx); viral (nonspecific); fungal; granulomatous (tuberculosis, sarcoid); luetic
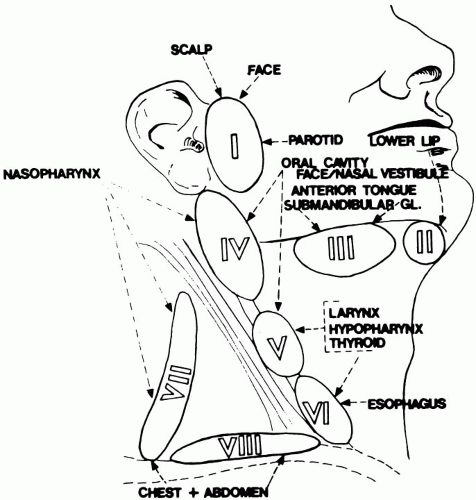
Location of the mass. Masses that are inflammatory or neoplastic usually follow the drainage pattern for the lymphatic vessels of the neck. The location of the mass may reflect the site of a primary infection or tumor. In general, the posterior cervical chain of lymph nodes drains the nasopharynx,
Waldeyer’s ring and sinuses. The anterior cervical chain drains the upper aerodigestive tract, from oral cavity to esophagus, running from superior to inferior. Supraclavicular nodes may drain the lower areas of the larynx and hypopharynx but also may represent the spread of a tumor from distant areas below the clavicles, including lung, breast, gastrointestinal tract, and kidney (Fig. 33-1). Midline neck masses are most frequently thyroid or congenital in origin.
Pain. Tender masses, especially if associated with systemic signs of infection, usually are inflammatory. Tenderness, however, may be absent with atypical mycobacterial adenitis despite overlying skin erythema. Tumor masses may be tender if they have become centrally necrotic or infected.
Mobility. Benign or inflammatory masses are usually mobile, although severe inflammation may cause a node to become adherent to adjacent structures. Fixed masses are more likely to represent malignant processes.
FIG. 33-1. Common drainage patterns of head and neck lymphatics. (Modified from Moloy P.How to (and how not to) manage the patient with a lump in the neck: common problems of the head and neck region. Washington, DC: American Academy of Otolaryngology—Head and Neck Surgery Foundation, 1986:9-30, with permission.)
Consistency. Soft masses in the neck often represent congenital cystic lesions or other benign lesions such as lipoma, lymphangioma, or hemangioma. Firmer, rubbery masses may be benign or inflammatory in nature, but they may represent a lymphoproliferative disease. Although a benign disease, toxoplasmosis can cause hard nodes that simulate malignant growth. Hard masses are more likely to be neoplastic.
Overlying skin. Painless fixation of the overlying skin to the mass indicates an infiltrative process or malignant growth. A punctum, dimple, or sinus tract may occur with branchial anomalies and sebaceous or dermoid cysts.
TABLE 33-2. Ancillary testing in diagnostic workup for neck mass
Test
Diagnostic information
Hematologic
Complete blood cell count with differential (CBC with diff)
Systemic infection, hematologic malignancy
Erythrocyte sedimentation rate (ESR)
Nonspecific elevation by systemic infection or tumor
Monospot (Epstein-Barr virus)
Infectious mononucleosis
Venereal Disease Research Lab (VDRL) and fluorescent treponemal antibody absorption (FTA-ABS)
Luetic adenitis
Angiotensin converting enzyme (ACE)
Elevated in sarcoidosis
Radiologic
Chest radiographs (CXR)
Granulomatous disease sarcoid, tuberculosis; pulmonary metastases from head and neck primary
Sonograms
Differentiate cystic and solid masses
Thyroid scan
Primary lesion
Computed tomography (CT) with contrast
Identify lesion from skull base to thoracic inlet
Magnetic resonance imaging (MRI)
Enhanced resolution of soft tissue structures compared to CT; without iodizined contrast. Multiple imaging planes, and for patients with renal insufficiency
Positron emission tomography (PET)
May aid in the diagnosis of malignant neck masses
Miscellaneous
Purified protein derivative (PPD)
Tuberculosis
Fine needle aspiration (FNA)
Cytologic biopsy of mass
Only gold members can continue reading. Log In or Register to continue