Neck
The neck distinguishes the head from the torso or trunk. Neck masses in children are common and usually represent cervical adenopathy that requires no intervention. However, in some instances, the nodes become large enough to cause suspicion of malignancy.
27-1 Lymph Node Excision
Introduction
Cervical adenopathy is common in children and usually requires no intervention. However, in some instances, the nodes become large enough to cause suspicion of a malignancy. In those instances, excisional (if possible) biopsy of an enlarged node is indicated.
Indications
The presence of a suspicious enlarged lymph node is the indication for excision of the mass.
Preoperative Evaluation
A computed tomography (CT) scan or magnetic resonance imaging (MRI) is helpful if the lymph node is large or if there are numerous nodes over the cervical region. A chest X-ray is indicated if there is suspicion of a malignant process in the neck. If there is a strong suspicion of a malignancy, the oncologist should be notified and prepared to perform a lumbar puncture and/or bone marrow aspirate if a malignancy is confirmed or suspected on frozen section evaluation of the node.
Operative Technique
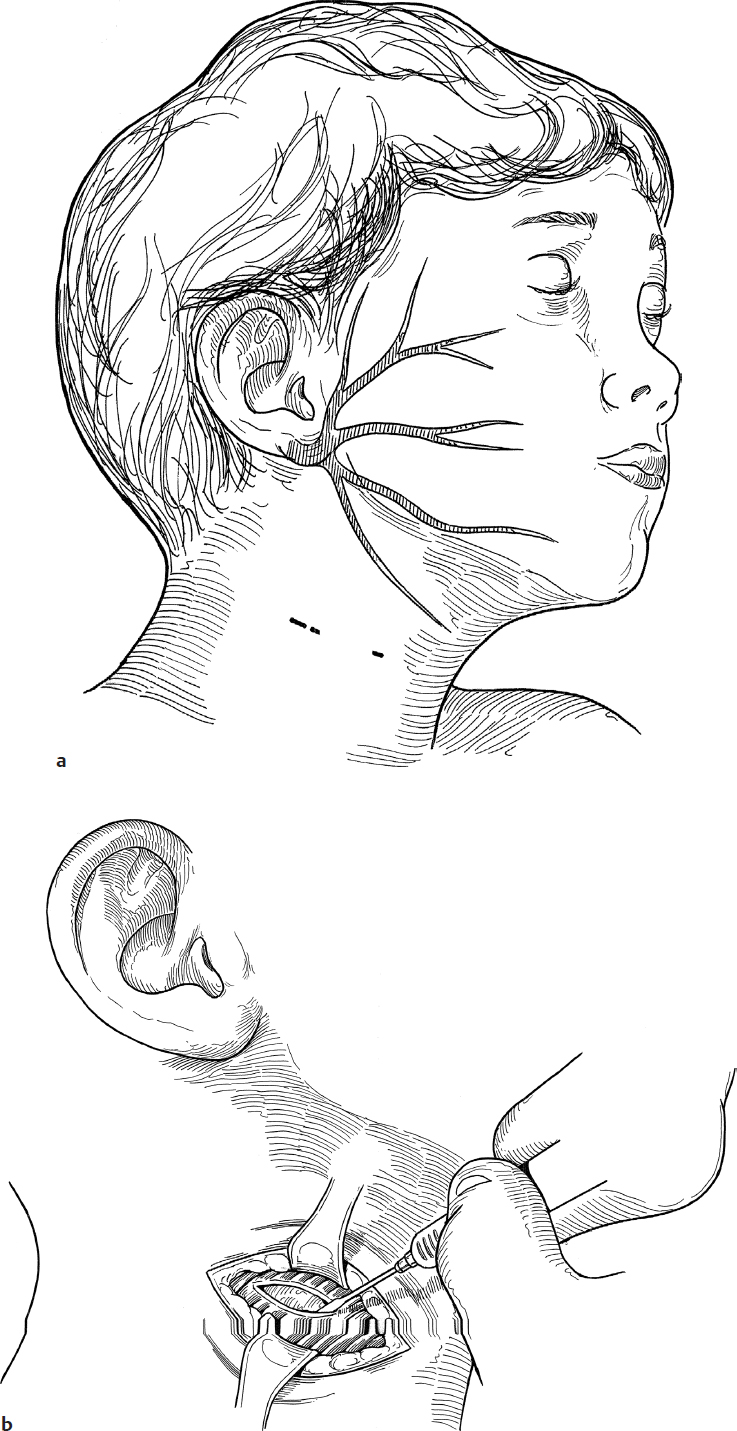
1. An appropriate transverse skin crease overlying the lesion and approximately 1.5 cm below the margin of the mandible is selected. Care is taken to stay away from the course of the marginal mandibular nerve. One percent lidocaine with 1:100,000 epinephrine is injected to help in hemostasis.
2. An incision is made with a no. 15 scalpel through the skin and subcutaneous tissue (Fig. 27.1a).
3. The platysma muscle is incised using the cutting cautery to reduce bleeding (Fig. 27.1b).
4. Soft tissue overlying the node (or nodes) is gently dissected off using fine pick-ups and delicate scissors. A small gauze peanut may be helpful in this maneuver.
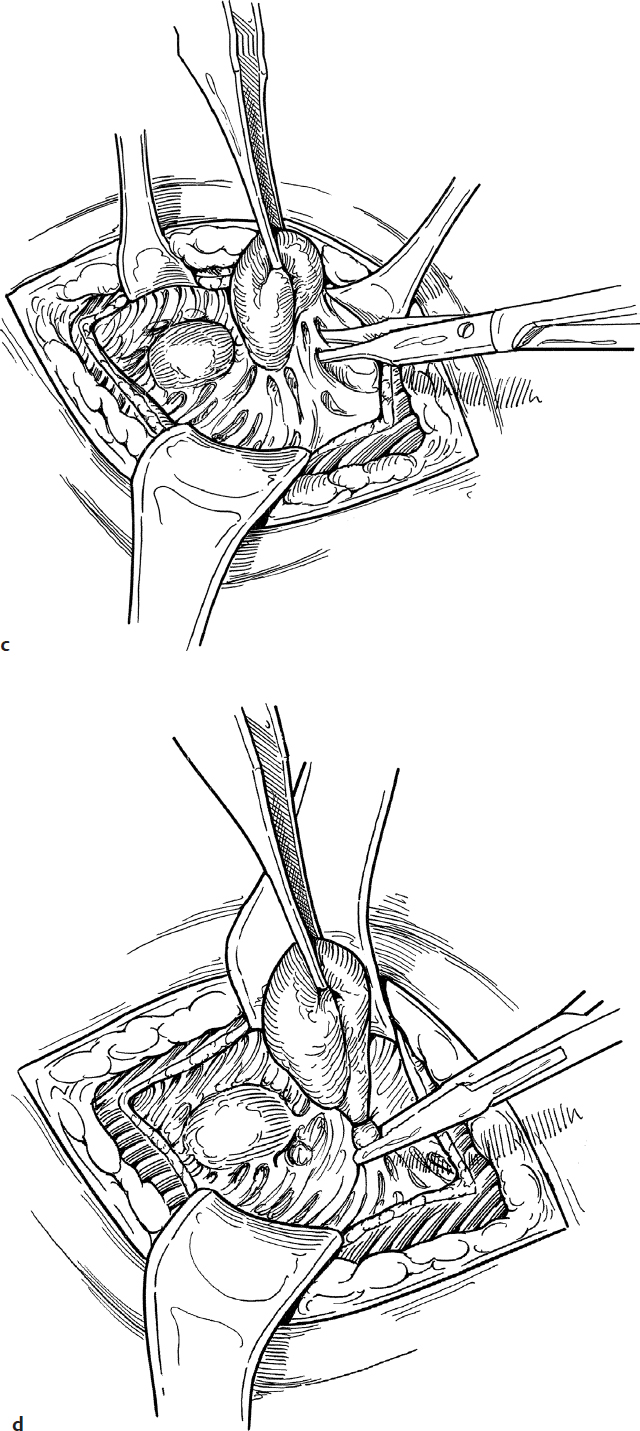
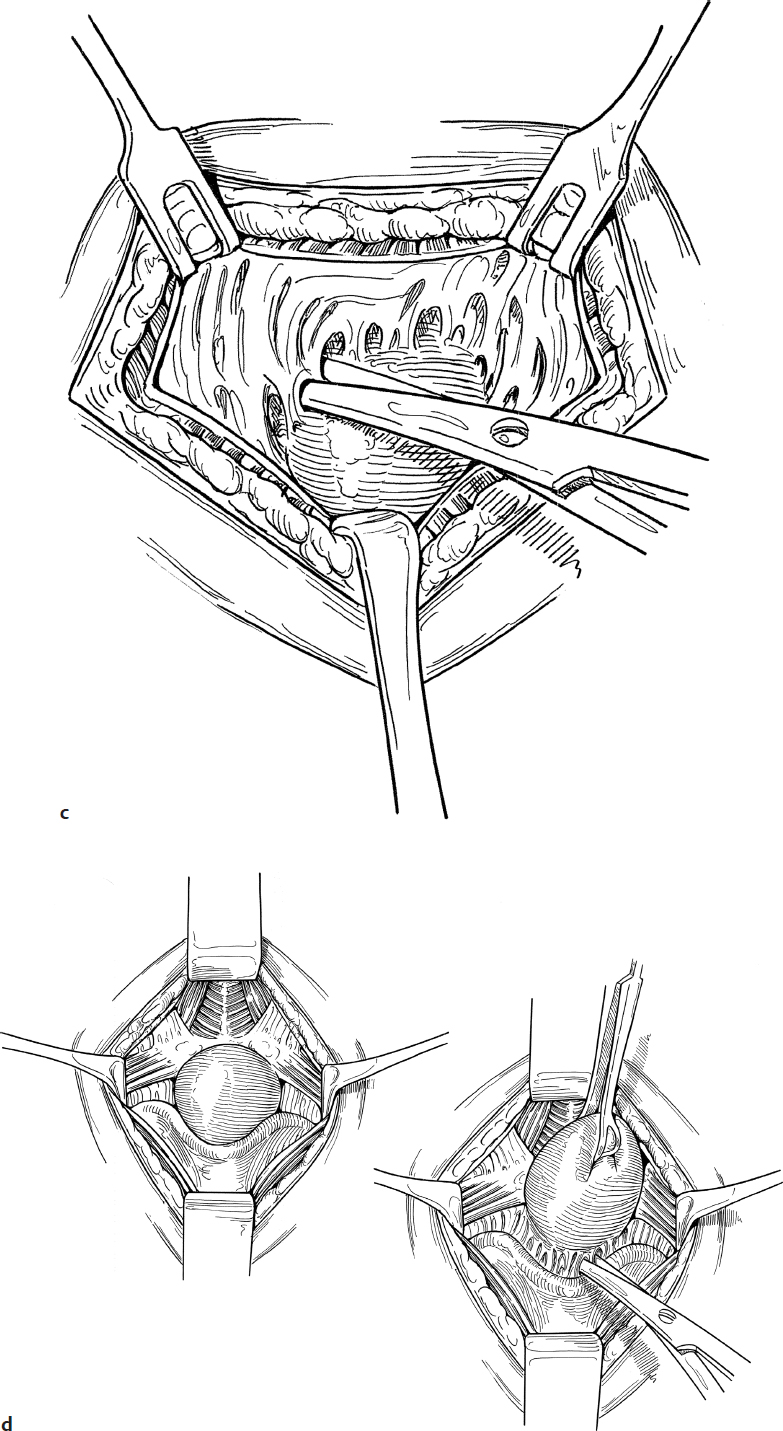
5. The node is gently grasped with fine forceps and dissected away from surrounding tissue with blunt and sharp dissection. Scissors are used to spread and then cut thin fibrous attachments. Every attempt is made to remove an intact node (Fig. 27.1c).
6. If a vascular pedicle is identified, this is clamped, cut, and tied with a 3-0 chromic suture (Fig. 27.1d).
7. If there is clinical suspicion of an infectious etiology for the node, a small piece is excised and sent for aerobic, fungal, and acid-fast cultures.
8. The node with its intact capsule is sent in a fresh state to the pathologist so that appropriate touch preps and stains may be performed.
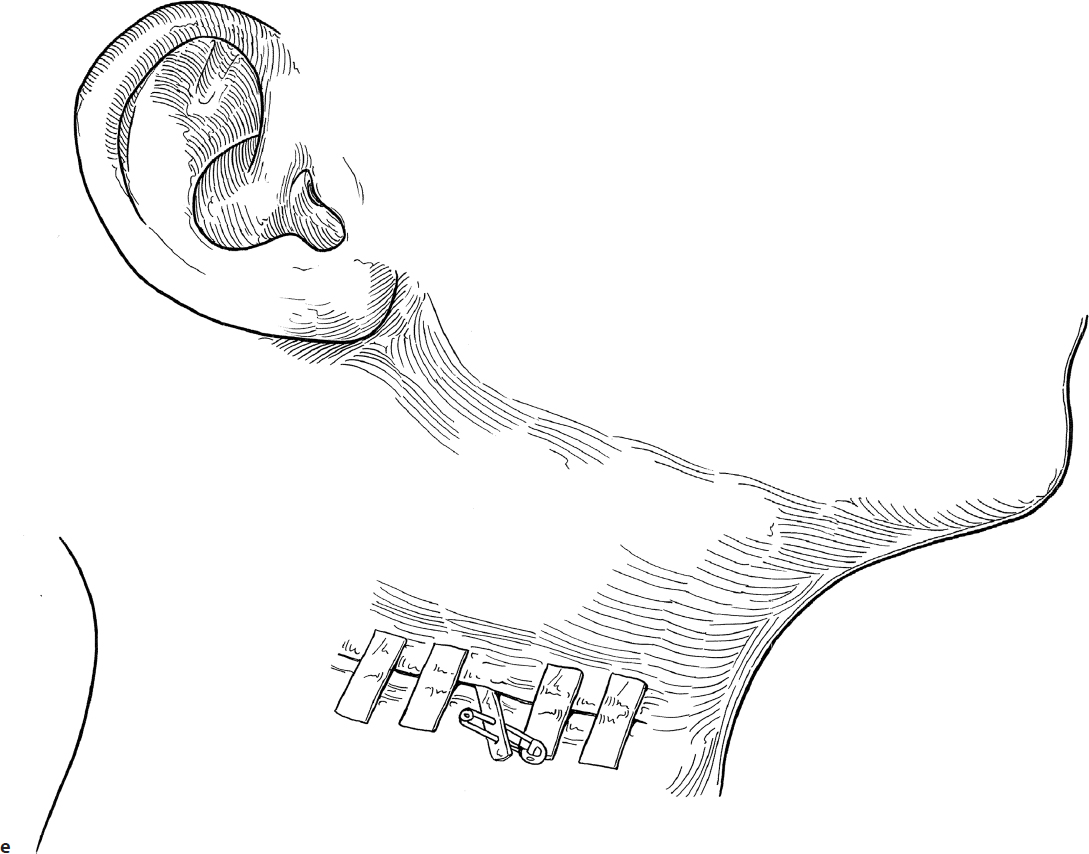
9. A small rubber band drain is usually placed to prevent accumulation of fluid and/or blood in the dissected cavity. A safety pin or suture is attached to the distal end of the drain to prevent it from being lost in the wound. The drain is removed within 24 hours.
10. The wound is closed in layers. The skin is closed with subcuticular sutures, and Steri-Strips (3M) are applied to keep the wound edges approximated (Fig. 27.1e).
Complications
1. Hemorrhage from a major vessel
2. Marginal mandibular nerve injury
27-2 Excision of Thyroglossal Duct Cyst
Introduction
A cervical thyroglossal duct cyst may occur anywhere from the base of the tongue to the lower third of the neck. They usually lie close to the midline.
Indications
Excision of a thyroglossal duct cyst is indicated before it becomes infected. Once infected, excision is associated with a higher rate of recurrence.
Preoperative Evaluation
A thyroid ultrasound to establish the presence of thyroid tissue in its normal location should be done prior to surgery. If the thyroglossal duct cyst contains the child’s only functioning thyroid tissue, thyroid replacement therapy will be required after excision.
Operative Technique
1. Excision of a thyroglossal duct cyst is performed under general anesthesia. One percent lidocaine with 1:100,000 epinephrine is injected to help with hemostasis.
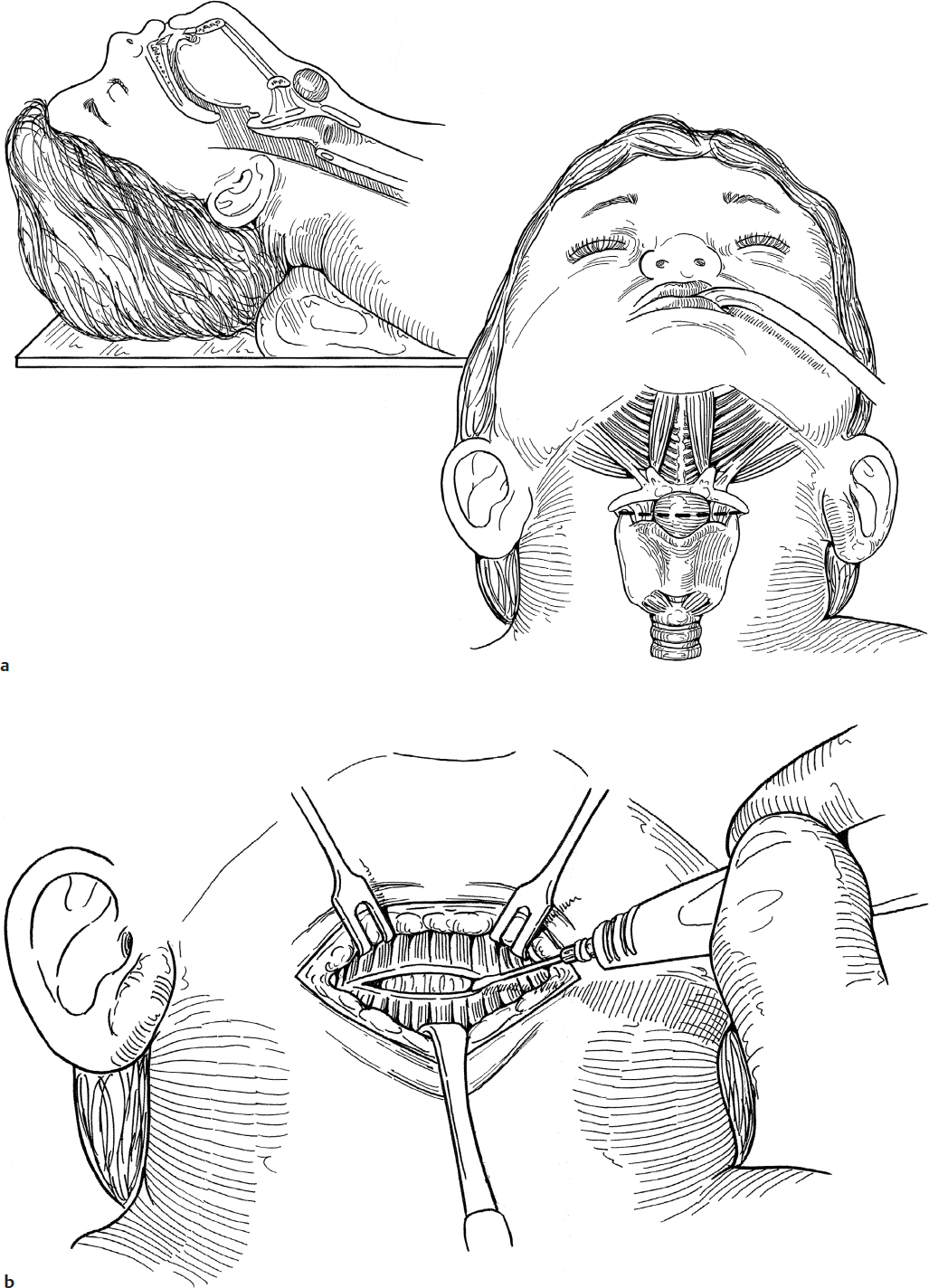
2. The child is positioned supine on a shoulder roll with the neck extended (Fig. 27.2a).
3. A transverse incision is made over the cyst through the skin, subcutaneous tissues, and platysma muscle with a knife (Fig. 27.2b).
4. Subplatysmal flaps are elevated with a scissors to a level above the hyoid bone and inferiorly to expose the cyst while being careful not to enter it (Fig. 27.2c).
5. The cyst is dissected from its surrounding soft tissue attachments, including the thyrohyoid membrane (Fig. 27.2d).
6. If the tract enters the thyrohyoid membrane, it should be tied with suture, divided, and oversewn.
7. The cyst and its track usually extend to and are attached to the mid portion of the hyoid bone.
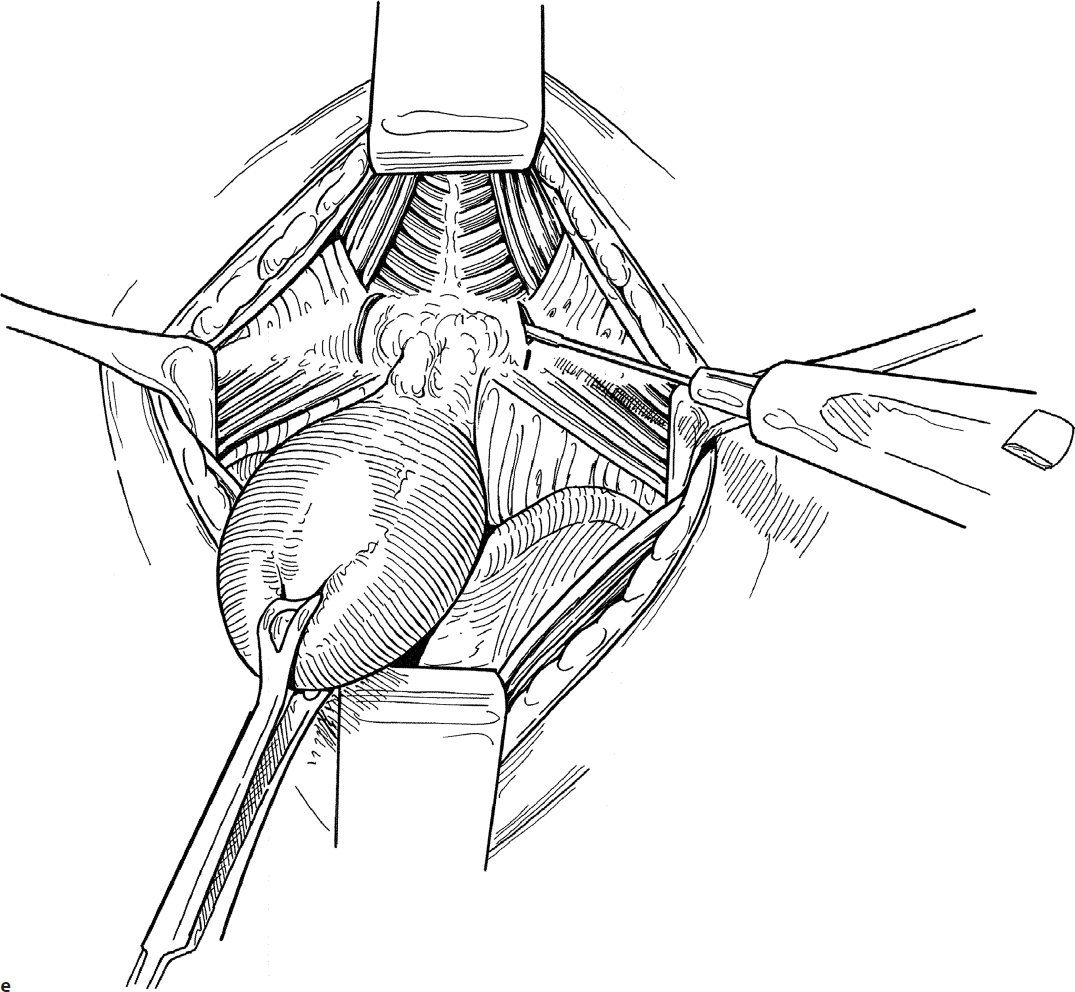
8. The hyoid bone is exposed laterally by cutting the overlying soft tissue with a knife or Bovie at the junction of the lesser and greater cornu (Fig. 27.2e).
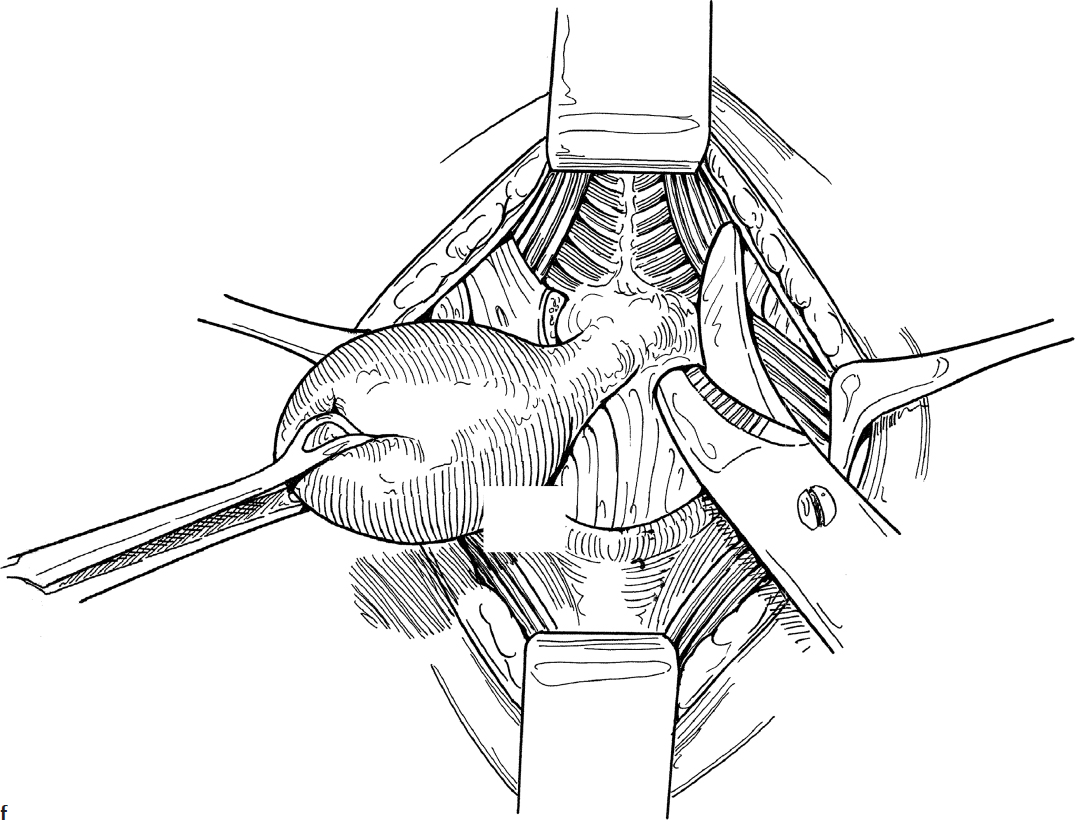
9. The hyoid bone is cut on each side at the lesser cornu with a bone cutter or heavy scissors (Fig. 27.2f).
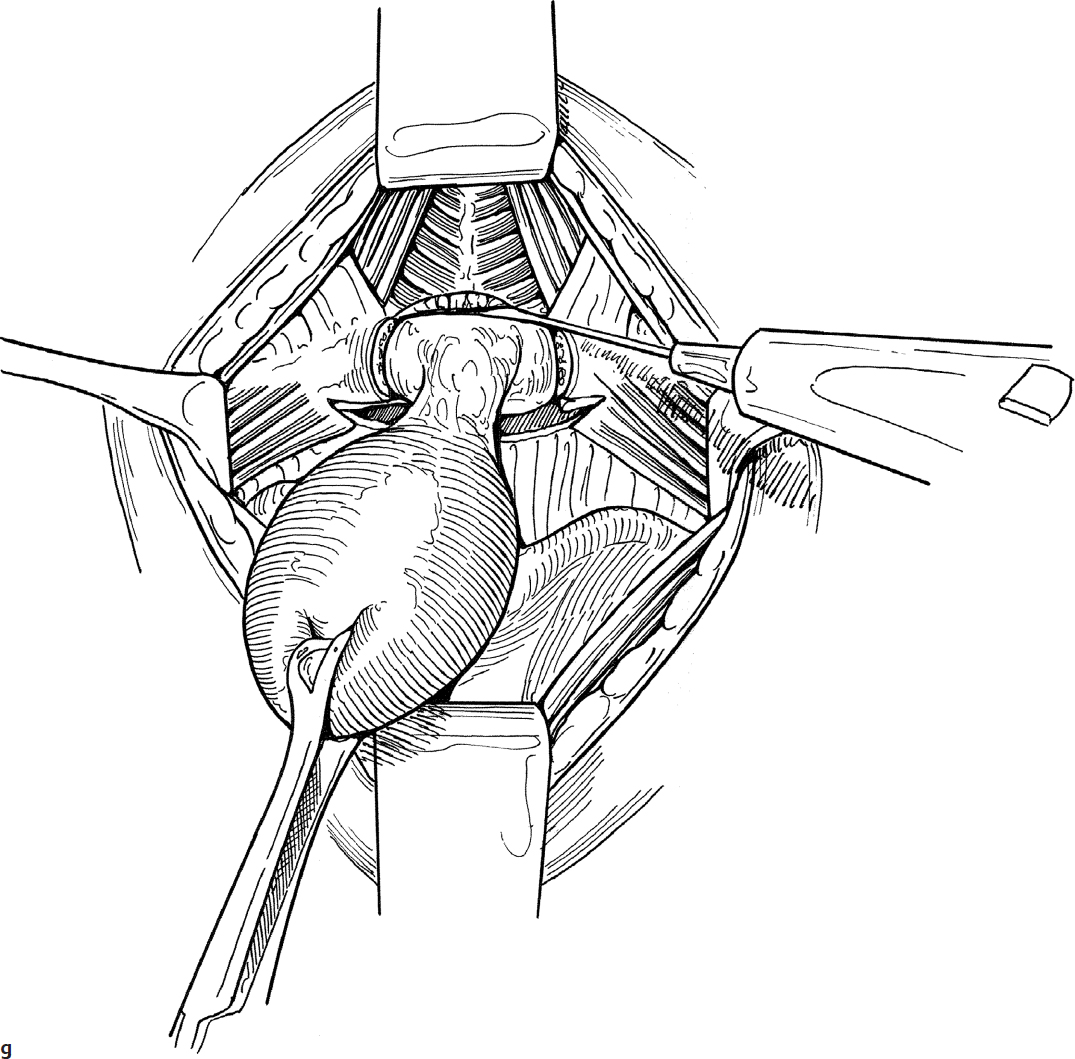
10. The superior and inferior muscle attachments to the hyoid bone are released with a knife or Bovie (Fig. 27.2g).
11. If a tract is present above the hyoid, it must be removed to prevent recurrence.
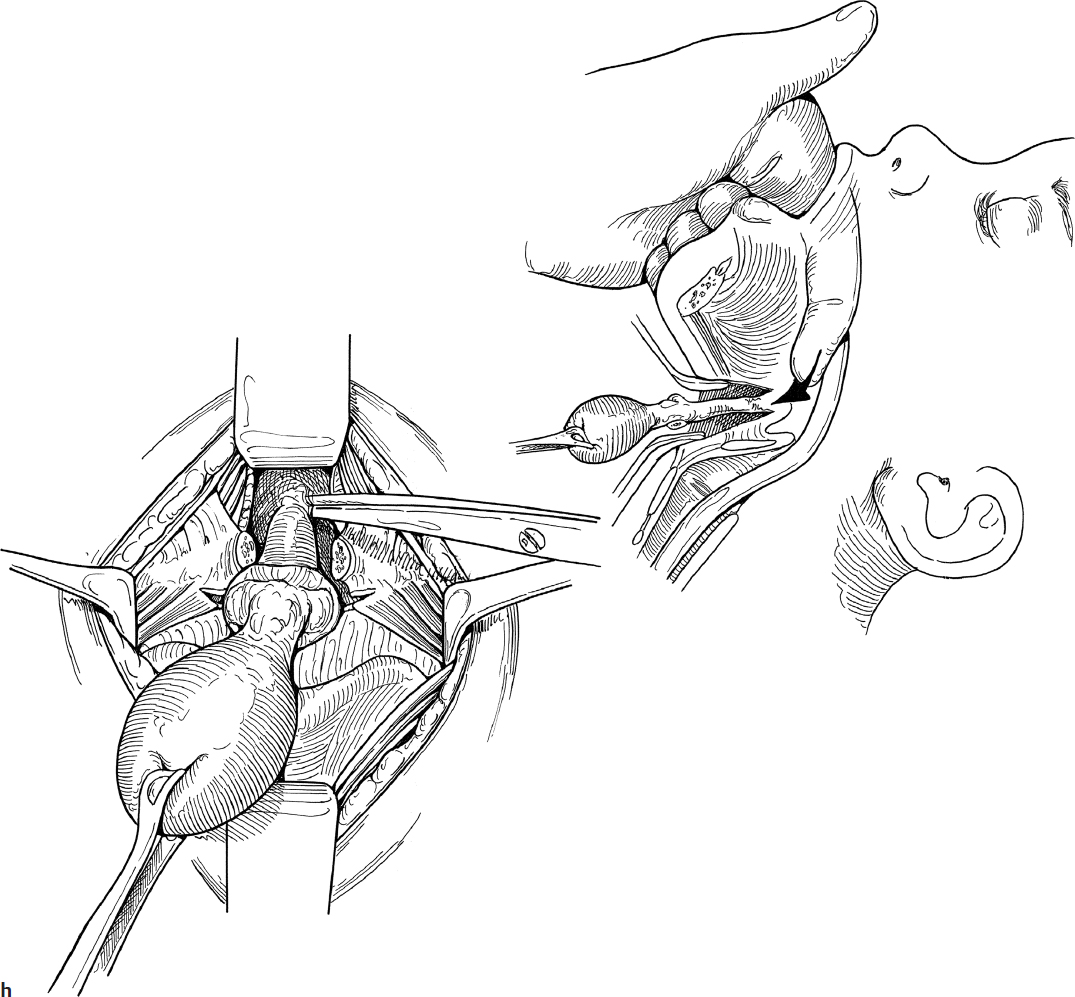
12. In some instances, it may be helpful for the assistant surgeon to break scrub to place the index finger of the left hand in the patient’s vallecula, and the base of the tongue is depressed into the surgical field. The core of soft tissue and tract are removed by sharp dissection with a scissors up to the foramen cecum (Fig. 27.2h). Complete excision of the tract rarely requires entering the oropharynx. If the pharynx is entered, one or two sutures of 3-0 chromic are usually all that is required to close the mucosal defect.
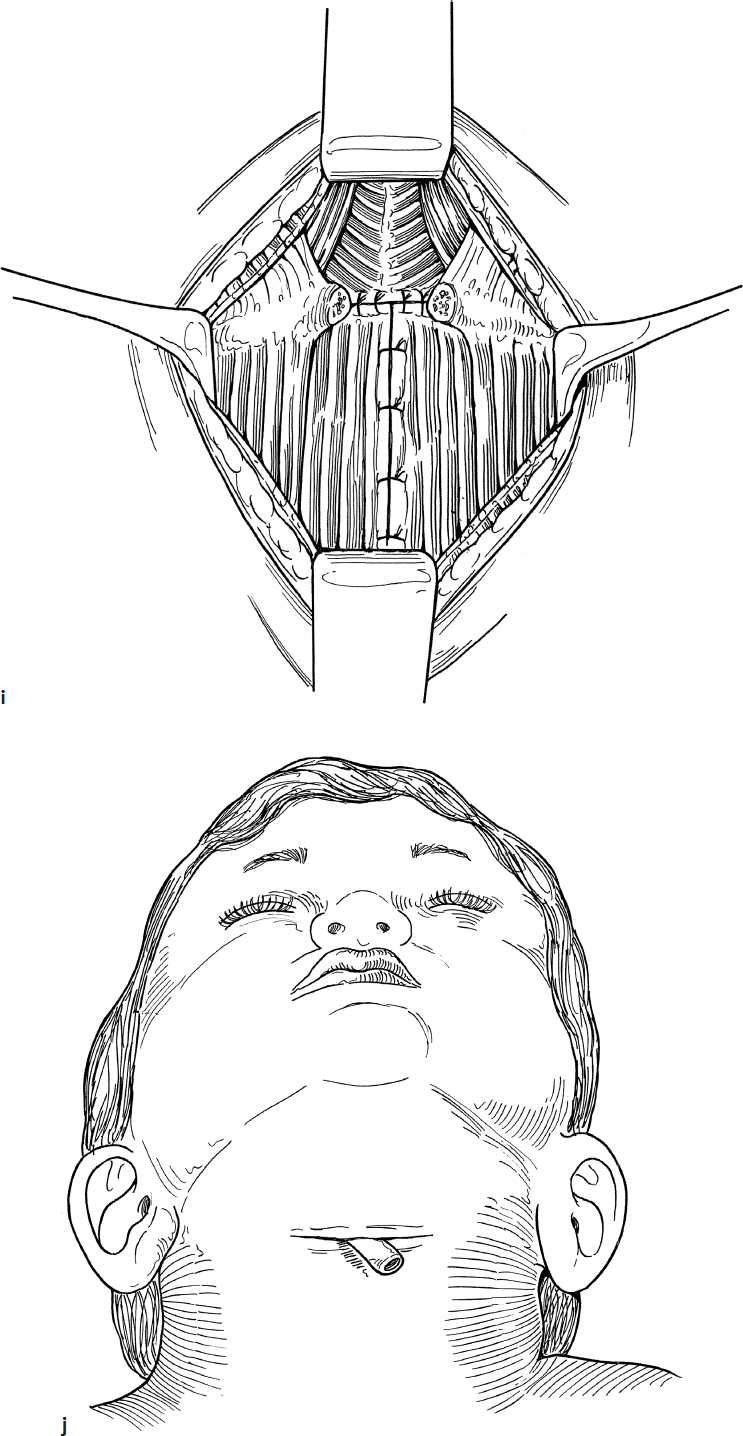
13. The wound is closed in layers with 3-0 chromic sutures to obliterate the dead space (Fig. 27.2i). A Penrose drain is placed in the wound and the skin may be closed with interrupted 5-0 nylon or subcuticular 4-0 Vicryl (Ethicon) (Fig. 27.2j). A light gauze dressing is applied.
14. Intravenous postoperative antibiotics should be administered until the drain is removed, usually 24–36 hours.
15. Oral antibiotics are used for 10 days.
Complications
1. Seroma
2. Cyst recurrence
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


