Purpose
To investigate the natural course of myopic traction maculopathy and to identify the factors associated with its progression or resolution in 207 highly myopic eyes.
Design
Retrospective, consecutive case series.
Methods
We investigated 207 highly myopic eyes with myopic traction maculopathy by optical coherence tomography (OCT) and followed the patients for at least 24 months. The size of the macular retinoschisis was categorized according to its extent and location relative to the fovea. The clinical data, status of the myopic traction maculopathy, and changes in the posterior vitreous and inner limiting membrane (ILM) were analyzed during the natural course of the disease process.
Results
During a mean follow-up of 36.2 ± 6.2 months, 8 of 207 eyes (3.9%) showed a decrease or complete resolution of the macular retinoschisis. Of these 8 eyes, 6 had release of retinal traction in the OCT images, and 4 of the 6 eyes developed posterior vitreous detachment. A spontaneous disruption of the ILM occurred in 2 eyes before the improvement of the myopic traction maculopathy. Of the 207 eyes, 24 (11.6%) experienced progression of the myopic traction maculopathy. The eyes with more extensive macular retinoschisis showed progression significantly more commonly (42.9%) than the eyes having less extensive macular retinoschisis areas (6.7%).
Conclusions
The natural course of myopic traction maculopathy varies, and eyes with more extensive macular retinoschisis tend to progress more commonly. A complete resolution of macular retinoschisis can occur after a release of traction on the retina. These findings can be used to determine whether surgery should be performed.
Myopic macular retinoschisis was first identified through the use of optical coherence tomography (OCT) by Takano and Kishi in 1999, and it was found in 9% to 34% of highly myopic eyes with posterior staphyloma. The terminology used in discussing this condition has not been consistent, and Pannozzo and associates proposed in 2004 to unify all of the pathologic features generated by traction in the myopic environment under the term myopic traction maculopathy . Eyes with myopic traction maculopathy include those with vitreomacular traction, retinal thickening, macular retinoschisis, lamellar macular hole (lamellar MH), and foveal retinal detachment (RD). Recently, Vanderbeek and Johnson reviewed the charts of 6 consecutive patients who had undergone vitreoretinal surgery for myopic traction maculopathy, and they found that the traction mechanisms causing the myopic traction maculopathy were diverse. Surgical repair of myopic traction maculopathy was successful both anatomically and visually when the major traction mechanism was relieved.
Eyes with myopic traction maculopathy have varying traction mechanisms and degrees of retinal damage, so it is to be expected that the prognoses will vary during the natural course of individual eyes. The natural course of macular retinoschisis has been studied in 8 eyes, 5 eyes, 21 eyes, 18 eyes, and 54 eyes. These studies have reported that the eyes with myopic macular retinoschisis can progress to more serious complications such as full-thickness MH and foveal RD during the follow-up period. On the other hand, Polito and associates reported one patient whose foveal RD and macular retinoschisis disappeared after a spontaneous posterior vitreous detachment (PVD) during the follow-up period. A PubMed search using keywords myopia and retinoschisis or foveoschisis or traction maculopathy identified no other publications reporting the spontaneous resolution of a myopic traction maculopathy.
The results of these studies suggested the possibility that the presence or release of a retinal traction might be related to the progression or resolution of a myopic traction maculopathy. However, most of these were small case series, and it has not been determined whether the natural course is affected by the degree or the extent of the macular retinoschisis. Also, the factors related to the progression or resolution of macular retinoschisis has not been investigated in a large series of patients with myopic traction maculopathy.
Thus, the purpose of this study was to determine the natural course of myopic traction maculopathy and to determine the factors that are associated with progression or resolution of the myopic traction maculopathy in 207 highly myopic eyes.
Methods
We retrospectively analyzed 207 highly myopic eyes of 168 consecutive patients with myopic traction maculopathy. The diagnosis of myopic traction maculopathy was made according to the criteria reported by Panozzo and associates. High myopia was defined as a myopic refractive error >–8 diopters (D) or an axial length >26.5 mm. These patients initially visited the High Myopia Clinic at Tokyo Medical and Dental University between January 8, 2008, and March 10, 2010, and were followed for at least 24 months. The patients with full-thickness MHs and those with histories of vitreoretinal surgery were excluded. Also, eyes with myopic choroidal neovascularization or a macular chorioretinal atrophy, which could affect the progression of myopic traction maculopathy, were also excluded. Approval by the Ethical Committee at Tokyo Medical and Dental University was obtained for this retrospective study.
The OCT examination was performed through a dilated pupil using the Cirrus HD-OCT (Carl Zeiss Meditec, Dublin, California, USA). In the OCT examination, the horizontal and vertical 5 scan lines were moved slowly while the scan monitor was viewed, and the images of the entire area of the macular retinoschisis were checked in detail. After the entire area of the macular retinoschisis was examined, the eyes were classified into 5 groups based on the size of the macular retinoschisis ( Figure 1 ; Table 1 ): no macular retinoschisis (S0); extra-foveal macular retinoschisis (S1); fovea-only macular retinoschisis (S2); foveal but not entire macular area macular retinoschisis (S3); and entire macular area macular retinoschisis (S4). This classification was based on the size of the outer schisis only; the size of the inner schisis was not considered.
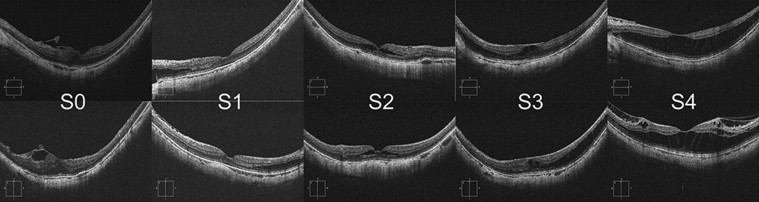
| S0 | Absent |
| S1 | Extrafoveal |
| S2 | Foveal only |
| S3 | Foveal but not entire macula |
| S4 | Entire macula |
Next, we determined whether other foveal pathologies were present on the OCT images—an inner lamellar MH, an epiretinal membrane, a vitreomacular traction, or a foveal RD. The fovea was identified as a depression of the inner retinal surface detected in the OCT images at the center of the macula, and its diameter was generally the same as that of an average optic disk (1.5 mm). The macular area was identified as a circular area centered on the fovea, and its diameter was 6 mm.
We analyzed the changes in the OCT findings during the follow-up period retrospectively. A resolution of myopic traction maculopathy was defined as a decrease in the height or extent of the macular retinoschisis without the development of an inner lamellar MH, foveal RD or full-thickness MH. A progression of the myopic traction maculopathy was defined as an increase in the height or extent of the retinoschisis or the development of an inner lamellar MH, foveal RD, or full-thickness MH. For the macular retinoschisis, an increase of more than 100 μm in height was considered an increase. For the macular retinoschisis area, an enlargement of the macular retinoschisis toward the area that did not have a macular retinoschisis was considered an increase. The eyes that did not meet the definition of a progression or resolution were classified as stable. All of the OCT images were examined by two of the authors (Y.T. and N.S.), and agreement by the two authors was needed to determine whether there was progression or resolution. The examiners were masked to the demographics of the patients. PVD was detected by OCT and was defined as a release of the attached posterior vitreous from the retina that occurred during follow-up.
Statistical analyses were performed using the Fisher exact probability test and the Mann-Whitney U test. P < 0.05 was considered significant.
Results
Clinical Characteristics
Among the 207 eyes of 168 consecutive patients, there were 56 men and 112 women with a mean age of 58 ± 11 years and a range of 30 to 79 years at the initial examination. The mean refractive error (spherical equivalent), except the 44 pseudophakic eyes, was −14.5 ± 3.6 D with a range of −6.0 to −23.0 D, and the mean axial length was 29.6 ± 1.5 mm with a range of 26.8 to 34.9 mm. The mean decimal best-corrected visual acuity (BCVA) was 0.81 with a range of 0.15 to 1.5. The mean follow-up period was 36.2 ± 6.2 months with a range of 24 to 48 months.
Among the 207 eyes, the macular retinoschisis of 32 eyes (15.5%) was classified as S0; that of 56 eyes (27.1%) as S1; that of 45 eyes (21.7%) as S2; that of 46 eyes (22.2%) as S3; and that of 28 eyes (13.5%) as S4. The 32 eyes with S0 included 27 eyes with only an epiretinal membrane and 5 eyes with subfoveal retinal thickness >200 μm but without evidence of a macular retinoschisis.
Natural Course of Myopic Traction Maculopathy
The baseline characteristics and the natural progression of the myopic traction maculopathy in each group, according to the macular retinoschisis area, are shown in Table 2 . There were no significant differences in age and axial length at the initial visit among the groups. The OCT findings at the initial examination showed that in 31 eyes, macular retinoschisis was classified as S2; in 8 as S3; and in 8 as S4; they all showed an inner lamellar MH in addition to the macular retinoschisis. A dome-shaped macula is an inward convexity of the macula caused by a localized variation in thickness of the sclera in the macular area of highly myopic eyes. A dome-shaped macula was found in 3, 4, 1, 4, and 2 eyes with S0, S1, S2, S3, and S4, respectively. There was no statistically significant difference in the BCVA at baseline or at the final examination in the 5 groups with S0 through S4.
| S0 a (32 eyes) | S1 a (56 eyes) | S2 a (45 eyes) | S3 a (46 eyes) | S4 a (28 eyes) | |
|---|---|---|---|---|---|
| Age (years), mean ± SD | 59 ± 10 | 52 ± 13 | 61 ± 10 | 59 ± 10 | 60 ± 10 |
| Axial length (mm), mean ± SD | 29.7 ± 1.6 | 30.2 ± 1.7 | 30.0 ± 1.6 | 30.0 ± 1.8 | 29.1 ± 1.1 |
| Inner lamellar MH at the first examination (eyes) | 0 | 0 | 31 | 8 | 8 |
| RD at the first examination (eyes) | 0 | 0 | 0 | 0 | 0 |
| DSM at the first examination (eyes) | 3 | 4 | 1 | 4 | 2 |
| Changes of OCT finding during a follow-up | |||||
| Improved | 0 (0%) | 1 (1.8%) | 1 (2.2%) | 3 (6.5%) | 3 (10.7%) |
| Decreased height or extent of macular retinoschisis | 0 | 0 | 0 | 0 | 2 |
| Complete resolution of macular retinoschisis | 0 | 1 | 1 | 3 | 1 |
| Stable | 30 (93.7%) | 53 (94.6%) | 40 (88.9%) | 37 (80.4%) | 13 (46.4%) |
| Progressed | 2 (6.3%) | 2 (3.6%) | 4 (8.9%) | 6 (13.0%) | 12 (42.9%) |
| Increased height or extent of macular retinoschisis | 2 | 2 | 2 | 6 | 9 |
| Development of inner lamellar MH | 0 | 0 | 1 | 0 | 2 |
| Development of FTMH | 0 | 0 | 2 | 0 | 0 |
| Development of foveal RD | 0 | 0 | 0 | 1 | 6 |
| BCVA (logMAR), mean ± SD | |||||
| First examination | 0.06 ± 0.18 | 0.05 ± 0.13 | 0.12 ± 0.25 | 0.09 ± 0.26 | 0.12 ± 0.28 |
| Final examination | 0.06 ± 0.20 | 0.05 ± 0.14 | 0.14 ± 0.27 | 0.10 ± 0.24 | 0.15 ± 0.28 |
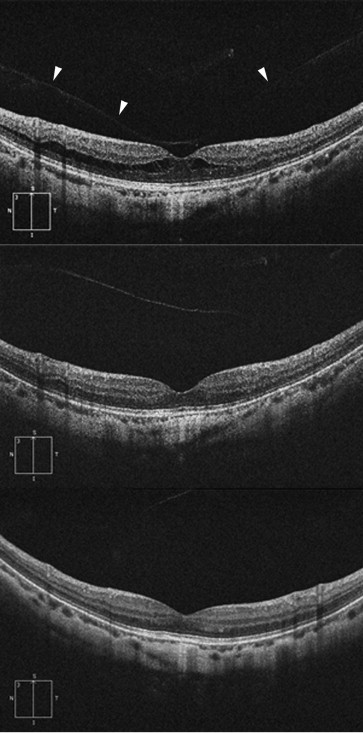
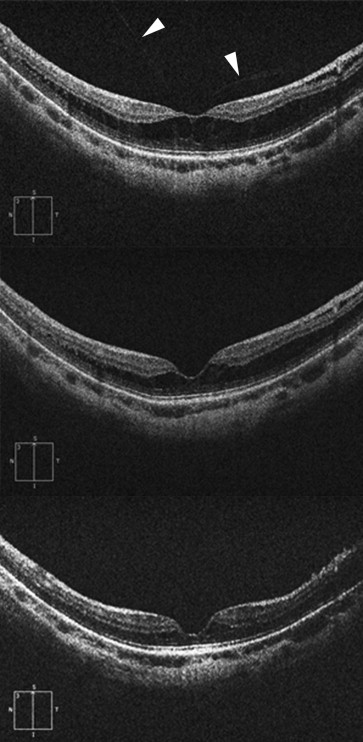
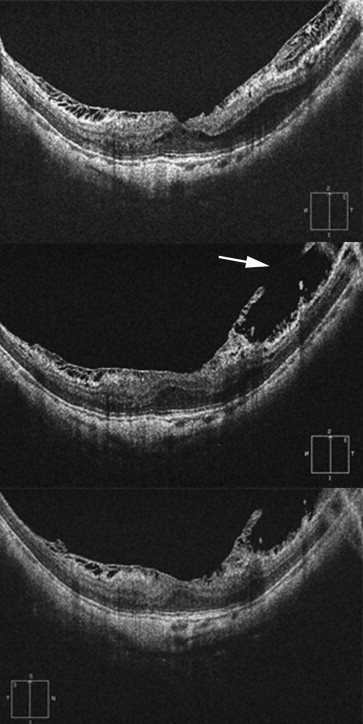
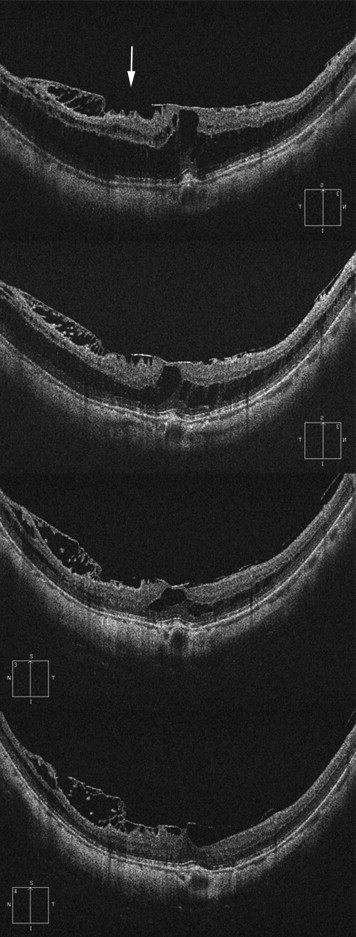
Among the 207 eyes with myopic traction maculopathy, 8 eyes of 8 patients (3.9%) experienced improvements in the OCT findings during the follow-up period ( Figures 2–5 ). The OCT-indicated changes in these 8 eyes included a decrease in the height or extent of the macular retinoschisis in 2 eyes and a complete resolution of the macular retinoschisis in 6 eyes. Improvements were found in none of the S0 eyes, in 1.8% of the S1 eyes, in 2.2% of the S2 eyes, in 6.5% of the S3 eyes, and in 10.7% of the S4 eyes. The differences in the rate of improvement in the 5 groups were not significant (Fisher exact probability test, P = 0.18).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


