Nasopharyngeal Stenosis
Nasopharyngeal stenosis usually occurs when there is extensive scarring following an adenoidectomy or adenotonsillectomy.
16-1 Repair of Nasopharyngeal Stenosis
Indications
Repair of nasopharyngeal stenosis is required to restore function of the upper airway impacted by obstruction at the junction of the nasopharynx and oropharynx.
Preoperative Evaluation
Flexible nasopharyngoscopy or indirect mirror nasopharyngoscopy is used to define the extent of the stenosis. In selected patients, computed tomography scans and magnetic resonance imaging are used to more thoroughly visualize the stenosis.
Operative Technique
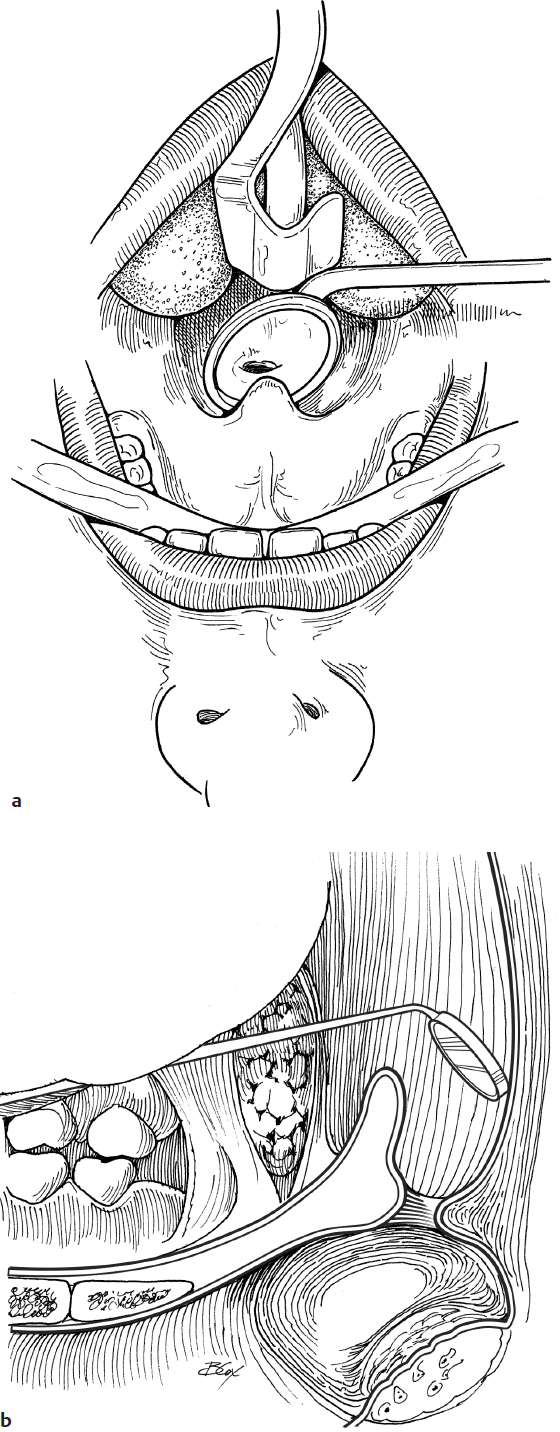
1. Repair of nasopharyngeal stenosis is carried out under general endotracheal anesthesia through an oral RAE tube with a mouth gag in place to expose the pharynx (Fig. 16.1a).
2. The nasopharyngeal lumen is visualized with a nasopharyngeal mirror (Fig. 16.1b).
3. If a lumen is present, nasal catheters are passed through the nasopharyngeal stenosis into the hypopharynx. They are then pulled out of the mouth to exert tension on the stenosis (Fig. 16.1c).
4. One percent lidocaine with 1:100,000 epinephrine is injected into the proposed incision lines (Fig. 16.1d).
5. Scar bands are divided to free the soft palate from the posterior and lateral pharyngeal walls (Fig. 16.1e).
6. Local mucosal flaps are rotated into the surgical defect (Fig. 16.1f).
7. Donor sites are closed as much as possible. Raw surfaces on the soft palate may be oversewn (Fig. 16.1g,h).
8. Kenalog-40 injections (Bristol-Myers Squibb) should be considered to control scar formation and restenosis.
9. A nasal endotracheal tube may be used to stent the nasopharynx open (Fig. 16.1i).
Complications
Restenosis of nasopharynx