Nasopharyngeal Angiofibroma
Nasopharyngeal angiofibromas, or juvenile nasopharyngeal angiofibromas (JNAs), are the most common benign neoplasms of the nasopharynx. They comprise approximately 0.5% of all head and neck neoplasms. They are unencapsulated vascular tumors composed of an irregular network of blood vessels in a fibroblastic stroma. These tumors are usually locally aggressive and destructive. JNAs also have the tendency to spread submucosally along lines of least resistance making assessment of their extent more challenging. Expansion of these tumors can occur anteriorly into the nasal cavity, posteriorly into the nasopharynx and sphenoid sinus, superiorly extending intracranially and into the cavernous sinus, and laterally into the pterygopalatine and infratemporal fossa. As they are extremely vascular tumors, patients with these tumors can have life-threatening epistaxis and massive hemorrhage intraoperatively.
JNAs present almost exclusively in adolescent males usually 10 to 17 years of age with a mean age at presentation of about 13 to 14 years. Nasal congestion and spontaneous epistaxis are the most common symptoms. Other less common symptoms include headache, facial pain, facial or cheek swelling, eustachian tube dysfunction and conductive hearing loss, trismus and jaw dysfunction, hyponasal speech, vision changes, proptosis, diplopia, and eyelid edema. Symptoms commonly present for 6 to 12 months prior to diagnosis.
Diagnosis is confirmed by imaging, most commonly computed tomography (CT) with contrast. JNAs have a classic appearance of a mass widening the space between the posterior maxillary wall and the pterygoids. Also, the mass demonstrates a rapid blush and enhancement after contrast administration. CT is useful in revealing the anatomic extent of the mass and its relationship to the bony anatomy of the nasopharynx and skull base. Magnetic resonance imaging (MRI) with contrast is also useful in determining the extent of the tumor. MRI can help delineate between soft tissue and fluid and assess the extent of tumor into the orbit and cavernous sinus as well as intracranially; vascular structural integrity and anatomy can also be assessed by MRI.
The author uses the Snyderman Classification System, described in 2010, which takes into account changes that arise as a result of the development of endonasal techniques.
Snyderman noted that tumor size and extent are less important in predicting complete tumor removal with endonasal surgical approaches. Using his classification system, sinus involvement is not considered an impediment to compete surgical resection. However, he did note two important prognostic factors predicting complete tumor removal and risk of recurrence: (1) route of cranial base extension; and (2) vascularity, in particular, residual vascularity after embolization. This system also provides better prediction of the immediate morbidity of blood loss during surgery, the need for multiple procedures, and risk of tumor recurrence.
In the new Snyderman Classification System, tumors are divided into five stages. Stage I is confined to the nasal cavity without extension lateral to the midpoint of the pterygopalatine fossa; stage II extends into the paranasal sinuses and/or lateral to the midpoint of the pterygopalatine fossa, without residual vascularity after embolization; stage III tumors exhibit skull base erosion or extension into extracranial spaces such as the orbit or infratemporal fossa, without residual vascularity after embolization; stage IV tumors exhibit skull base erosion and/or extension into the orbit and/or infratemporal fossa, with residual vascularity after embolization; and, lastly, stage V tumors exhibit intracranial extension and residual vascularity. Stage V lesions are also separated into M type tumors with medial routes of extension (cavernous sinus and medial to the paraclival and cavernous segments of the internal carotid artery) and L type tumors with lateral routes of extension (middle fossa superior to the petrous portion of the internal carotid artery and lateral to the paraclival and cavernous segments of the internal carotid artery).
Surgery is the primary treatment modality and performed completely endonasal, endoscopically assisted, or via an open approach. Other treatment modalities that have been utilized include radiotherapy, hormonal therapy, and chemotherapy. Traditionally, large or extensive JNAs were considered to require open approach for resection, while endonasal approaches were reserved for smaller of more limited JNAs. Open approaches include lateral rhinotomy, transpalatal, transmaxillary, midfacial degloving, Lefort I, Weber-Fergusson, and cranio-zygomatico-facial.
15-1 Excision of Nasopharyngeal Angiofibroma
Indications
Nasopharyngeal angiofibromas are excised to prevent recurrent epistaxis, nasopharyngeal obstruction, and intracranial extension.
Preoperative Evaluation
The preoperative evaluation of a nasopharyngeal angiofibroma includes CT scan, MRI with MR angiogram, and arteriography with arterial embolization. Embolization is usually performed 24 to 72 hours prior to resection to reduce intraoperative blood loss.
Operative Technique
With the development of endonasal techniques and technologies, the endonasal approach has expanded to include resection of larger lesions. Often, lesions that were once considered to be only amenable to open resection can be managed either completely endonasally or by an endoscopic-assisted approach (see Section 13-1).
Endonasal approaches have been made possible in part by the preoperative embolization of these tumors to reduce their vascularity. Preoperative embolization may reduce intraoperative blood loss and improve visualization during endonasal procedures. Angiography with embolization is typically utilized prior to surgery; however, there have been descriptions of use of direct injection of materials into the JNA, during surgery, to embolize the tumor. One such material is an ethylene vinyl alcohol copolymer, Onyx, which can be directly injected into a lesion under fluoroscopy to see its extension into the tumor.
Endoscopic resection of JNAs has the benefits of better illumination, magnified and panoramic views, ability to visualize around corners and edges, less morbidity, no cutaneous incisions, and reduced hospitalization. However, some of the disadvantages of the endoscopic approach include: visualization through the scope is easily obscured by blood in the field, may require an additional skilled assistant, and limited access in the case of massive bleeding. A surgeon can consider converting a completely endonasal technique to an endoscopically assisted one and widen access by combining the open approach, such as a Caldwell-Luc, to access some of the lateral extent of the tumor or gain an additional tunnel of approach to a deep lesion. One should be cautioned that, if an endonasal or endoscopically assisted approach is planned, the surgeon should be prepared and able to convert to an open approach, as well as having craniofacial and neurosurgical backup.
Endonasal approaches have essentially replaced lateral rhinotomy and transpalatal approaches especially for small to mid-sized tumors performed by endoscopically experienced surgeons. Even large, more extensive tumors are often able to be addressed using endonasal techniques.
Endonasal approaches have been made practical and an excellent choice for the management of JNAs because of preoperative embolization and technologies such as microdebriders, extended length drill burs, skull base burs, lasers, endoscopic bipolar forceps, and radiofrequency and plasma technology. Given that endonasal techniques have replaced open approaches for management of most JNAs, this approach is described here.
Endonasal Technique
1. Preoperative embolization within 24 to 72 hours prior to surgical resection.
2. Consider the use of an intraoperative computer-assisted guidance (IGS) system. Verify accuracy and review plan.
3. Begin in the nasopharynx.
a. Introduce a tonsil mouth gag (Dingman or Crowe-Davis) and suspend in the typical fashion as for an adenoidectomy.
b. Carefully introduce a 10-French catheter through the contralateral nostril and deliver it through the oral cavity. Approximate the two ends and apply a slight amount of tension to retract and elevate the palate. Then clamp the two ends of the catheter as to maintain this traction.
c. Using a dental mirror or angled endoscope, visualize the nasopharynx from the posterior/inferior aspect.
d. The posterior aspect of the JNA can be visualized and demarcated using a plasma wand, bipolar cautery, or a monopolar suction cautery, taking care to avoid injury to the tori. Sometimes the JNA can be submucosally attached to the septum and may need to be addressed there as well. Some debulking of the JNA may be performed from this direction. This will define the posterior extent of the resection of the JNA.
4. Debulk the nasal cavity component of the JNA. Protect normal mucosa and the nares as injury may be caused during the repetitive insertion and removal of the endoscope and instruments into the nasal cavity. By debulking the intranasal component, this will make further dissection easier and provide room to displace the tumor. Dissection around the tumor mass can be performed with a suction elevator and neurodissectors. Removal of tissue can be performed with a multitude of different methods such as bipolar and suction cautery, laser, or coblation.
5. Consider posterior septectomy. This will allow for exposure to the posterior aspect of the tumor through the contralateral nostril. Also if the septectomy is made large enough, visualization into the pterygoid fissure and lateral aspect of the sphenoid recess may be made easier from the more obtuse angle provided through the contralateral nasal cavity.
6. Clip and ligate the sphenopalatine artery.
7. An extensive maxillary antrostomy and removal of the posterior wall of the maxillary sinus provides additional exposure of the tumor. This can be performed using diamond burs and neurodissectors/elevators. The extended length and skull base burs are particularly useful to drill this bone. A wide maxillary antrostomy will allow better exposure to the posterior wall of the maxillary sinus and pterygomaxillary fissure and, in some cases, out into the medial aspect of the infratemporal fossa. This may allow adequate exposure to deliver a JNA that extends into the infratemporal fossa, maxillary sinus, and nasal cavity. The internal maxillary artery may also be visualized and ligated with endoscopic clip appliers and cut with endoscopic scissors.
8. Debulking the tumor will provide space into which the tumor may be displaced to allow it to be dissected out of various areas, such as the paranasal sinuses, the infratemporal fossa, the orbit, intracranially, and the cavernous sinus.
9. If more lateral access and exposure are required, one may consider a sublabial incision and create an opening in the face of the maxilla.
10. Control of posterior vascular supply.
a. If the mass goes posteriorly into the sphenoid sinus, the surgeon must pursue the lesion posteriorly. The extended length or skull base burs are helpful to remove the face of the sphenoid.
b. Care must be taken posteriorly as there is typically vascular supply from the Vidian artery. Drilling the sphenoid bone may allow this artery to be identified and managed.
c. Often there is vascular contribution that comes through the cancellous bone of the clivus and sphenoid bone. Drilling of the bone may be necessary to completely remove tumor extending into the bone, and then this may require hemostatic agents to be applied, such as bone wax, to control bleeding.
11. Superior extent
a. Cavernous sinus: If there is extension into the cavernous sinus, sometimes a plane may be created between the cavernous sinus and the JNA. Careful dissection may allow delivery of tumor that extends into the region of the cavernous sinus. Care should be taken to avoid penetrating or tearing the sinus. One needs to remember that this is a benign process and leaving a small amount of tumor adjacent to delicate structures may be better than causing significant morbidity.
b. Intracranial extension may often be brought inferiorly into the nasal cavity. The dura often provides a barrier to the JNA. Sometimes there is a thin rind of attenuated bone still remaining between the JNA and the dura, which can provide a plane of dissection. If there is a large skull base defect, a portion of septal bone or a split calvarial bone graft may be required to reconstruct the skull base.
12. At the completion of the procedure, the defect can be packed with hemostatic agents and antibiotic-coated gauze strip packing or Xeroform strips (Covidien). To help with breathing, a nasopharyngeal airway may be placed through the nose and have the packing around the airway, thereby allowing air to pass through the nose after surgery. Typically, the nasopharyngeal airway and packing are removed 2–3 days postoperatively.
13. The patient may require temporary placement of a ventilation tube in the ipsilateral ear if there is persistent fluid and conductive hearing loss.
Hemostatic Agents to Be Considered
1. Ephedrine: 1:1,000 topical application of Gelfoam (Pfizer) or Cottonoid neuropledgets (Codman). May consider coloring the liquid to help identify it and prevent inadvertent injection; can use methylene blue or fluorescein.
2. Gelfoam with thrombin
3. Surgicel (Ethicon)
4. FloSeal (Baxter)
5. Avitene (Davol Inc.)
6. Bone wax
Endoscopically Assisted Techniques
The surgeon may combine open exposures such as a Caldwell-Luc approach or midface degloving and translocation to gain more extended exposure and utilize endoscopic techniques to resect tumor that may otherwise have required a much more extensive approach in order to have direct line of sight exposure (see Section 13-1).
Open Approaches
Lateral Rhinotomy
Refer to Section 13-1, Lateral Rhinotomy.
Transpalatal Operative Technique
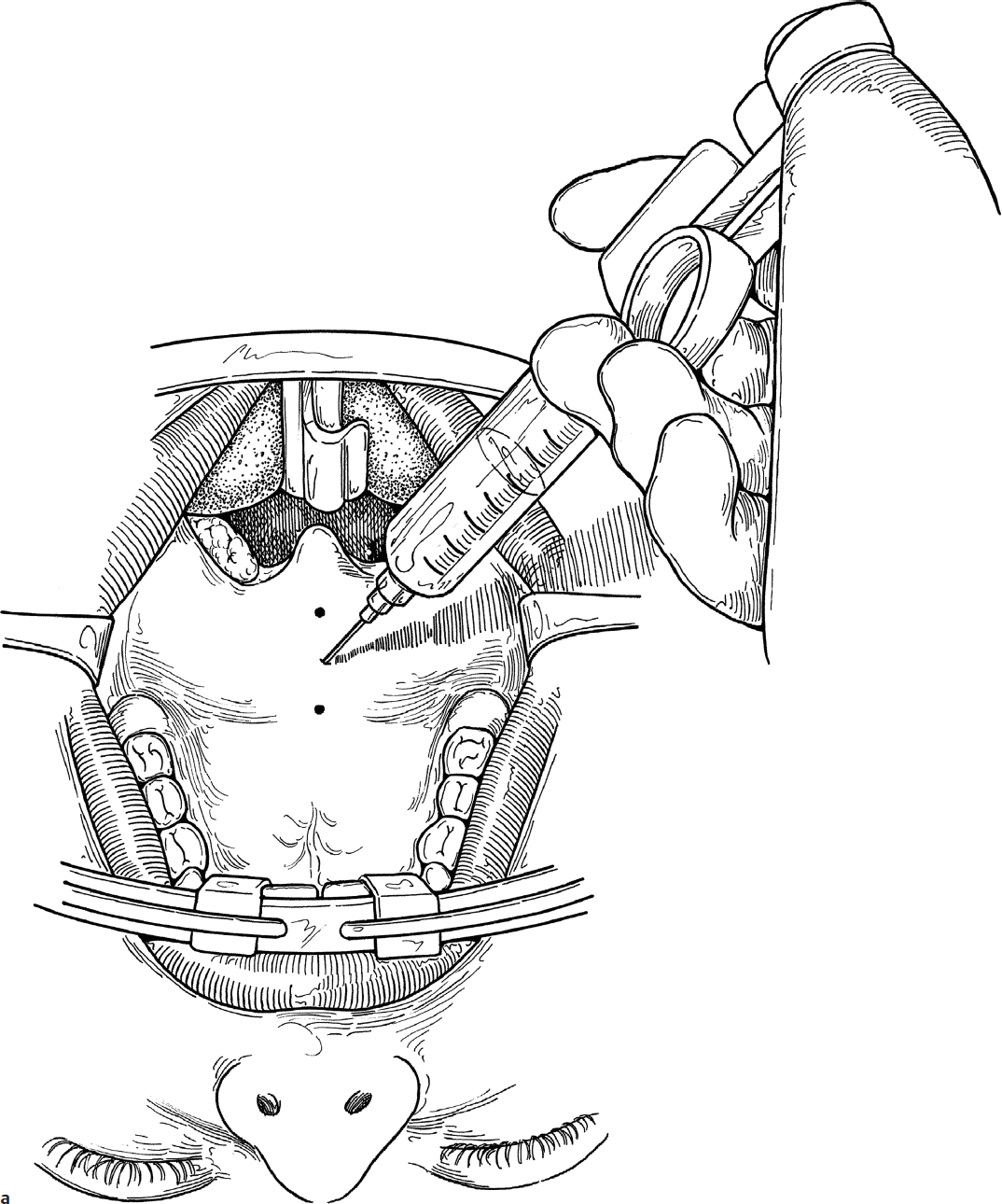
1. Transpalatal excision of an angiofibroma is performed utilizing general anesthesia administered through an oral RAE tube. A Dingman mouth gag is placed for exposure of the palate (Fig. 15.1a).
2. The midline of the palate is injected with 1% lidocaine with 1:100,000 epinephrine for hemostasis (Fig. 15.1a).
3. A midline palatal splitting incision is made with a knife through the soft palate and through the soft tissue overlying the hard palate (Fig. 15.1b). Incision can be made to one side of the uvula, rather than through the middle of the uvula.