Nasal Tumors
Nasal tumors span the full range of intranasal pathology, but the vast majority of intranasal tumors in children are benign.
13-1 Lateral Rhinotomy
Introduction
This is an open approach to provide exposure inside the nasal cavity. It may be combined with a medial maxillectomy to give excellent exposure to the lateral aspect of the nasal cavity and maxillary sinus, and even out laterally into the infratemporal fossa. Lateral nasal wall tumors and nasal septal masses can be approached via this method. However, with the advancement of endoscopic techniques and technology, the need for a lateral rhinotomy to manage intranasal lesions has decreased.
Indications
Lateral rhinotomy is indicated for a mass of the lateral wall of the nasal cavity or septum that may not be able to be managed or accessible by endoscopic techniques.
Preoperative Evaluation
Direct examination of the nasal cavity should be performed. A headlight with a nasal speculum and/or anterior rhinoscopy with an otoscope is useful in evaluating the anterior nasal cavity. The remainder of the nasal cavity and posterior nasal cavity may be examined using flexible or rigid endoscopy. Radiologic imaging is useful to delineate the anatomy and extent of the lesion. Computed tomography (CT) is useful to determine bony anatomy and can show signs of bony remodeling and/or erosion. Magnetic resonance imaging can help determine extent of the lesion and involvement of surrounding soft tissues.
Operative Technique
1. General anesthesia with an oral RAE tube.
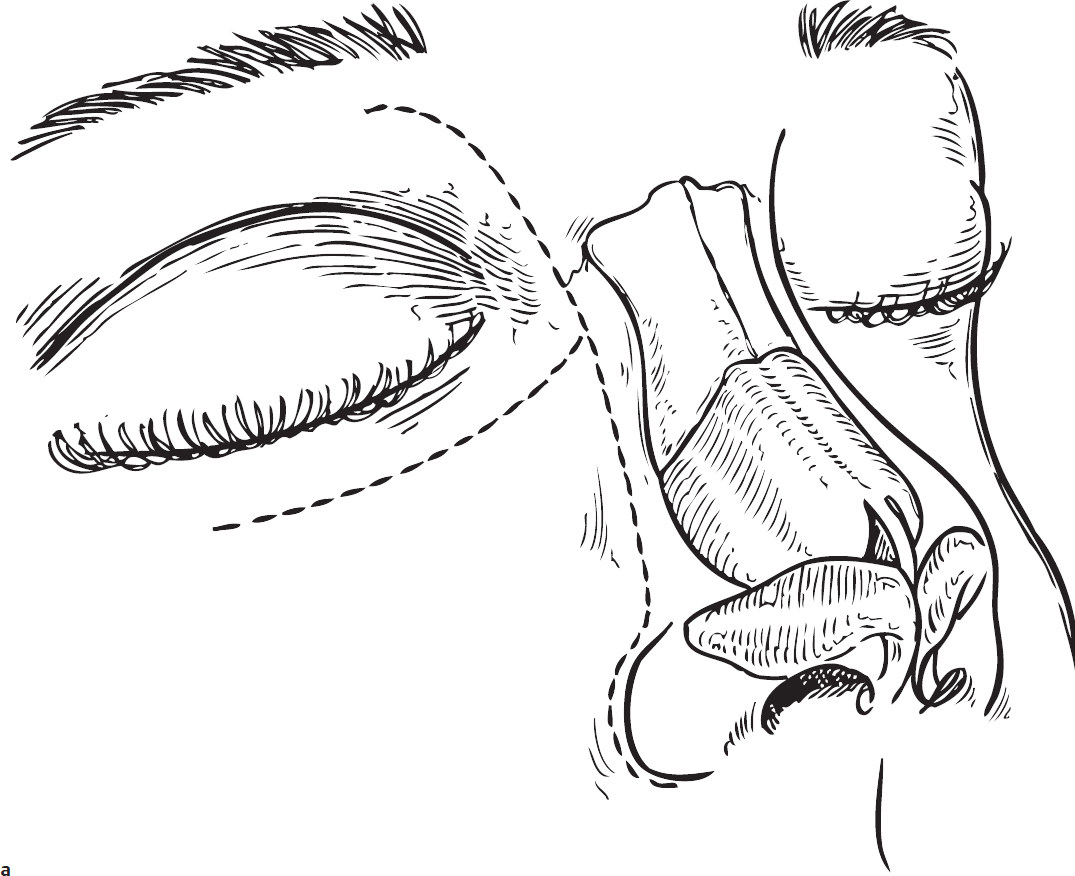
2. An incision line is drawn along the edge of the aesthetic unit between the cheek and the lateral aspect of the nasal dorsum. This is then extended down around the base of the nasal alae (Fig. 13.1a).
3. Injection of 1% lidocaine with 1:100,000 epinephrine is made along the planned incision line to aid in hemostasis.
4. An incision is made around the base of the nasal alae down to the edge of the pyriform aperture. The incision can be extended up along the lateral edge of the nose between the cheek and the lateral aspect of the dorsum of the nose (along the aesthetic unit). The incision can even extend up to the level of the medial canthus along a line one-half the distance between the medial canthus and the dorsum of the nose. Then the incision can be extended laterally through the medial canthus and along the inferior orbital rim. This will allow access to the ethmoid and the maxillary sinuses. A medial maxillectomy can also be performed through this incision (Fig. 13.1a).
5. From the edge of the pyriform aperture, a small osteotome can be used to cut along its lateral edge and then brought medially toward the dorsum at the junction of the nasal bone and the bony nasal septum. This will allow this piece of bone to be flapped medially allowing exposure to the nasal cavity (Fig. 13.1b,c).
6. The maxillary and ethmoid sinuses may be opened to provide lateral and posterior exposure, respectively. Bone can be removed with a drill or rongeurs (Fig. 13.1d).
7. If further exposure is required after opening the face of the maxilla, the medial aspect of the maxilla may be removed by creating osteotomies between the antral window and the opening created in step 5. This anterior medial buttress of the maxilla can be replaced at the completion of the case using plates or wire (Fig. 13.1e).
8. After the tumor is resected by sharp dissection with scissors or knife, the nasal bone can be returned to its normal position; it can be secured with a suture or small absorbable plate or supported intranasally with packing.
9. The incision is closed with 4-0 absorbable sutures in the subcutaneous layers and the skin closed with 5-0 interrupted subcuticular absorbable suture (e.g., Chromic gut [Ethicon] or Monocryl [Ethicon]) (Fig. 13.1f).
Complications
1. Nasal dorsal deformity
2. Nasal alar scarring/deformity
3. Incisional scar
4. Infraorbital nerve injury
5. Orbital hemorrhage/loss of vision/ophthalmoplegia
6. Cerebrospinal fluid leak