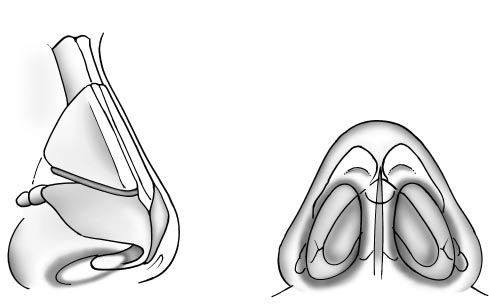
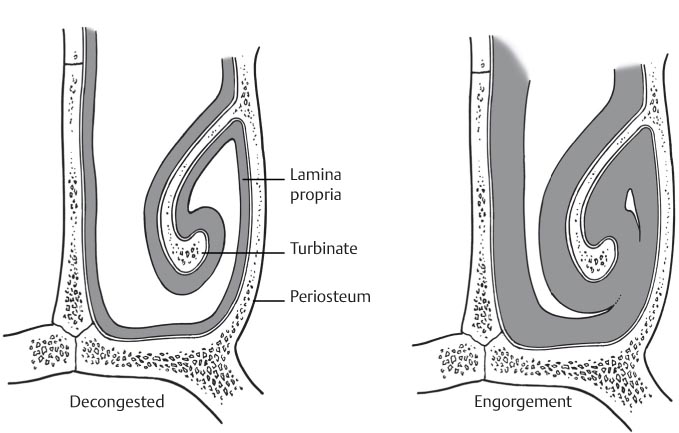
27 Nasal Obstruction The complaint of nasal airway obstruction arguably shares the most overlap between normal relatively mild and common disease states and more significant pathologic conditions. It therefore serves as an ideal example of the type of complaint that may require a thorough understanding of anatomical variances, physiology, and available diagnostic modalities required to differentiate its varied potential causes. The nasal cavity consists of a rigid or fixed framework that includes the bony lateral walls, cartilaginous septum, bony septum, and bony portions of the turbinate (Fig. 27.1). The narrowest portion of the nose is the anterior section from the nostrils to the piriform aperture. Any obstruction in the narrowest part of the nose will further the resistance to airflow and lead to nasal obstruction. There is also a significant dynamic component that may contribute to nasal blockage. The mucosal surfaces and the vasculature associated with these surfaces contribute to this variable portion. The nose, in particular, the turbinates, is lined by highly vascular mucosa, including the Kiesselbach plexus on the septum and cavernous tissue of the turbinates. Physiologic congestion, under the control of the autonomic nervous system, causes the nasal mucosa to congest and decongest in a cyclical side-to-side fashion. At any time, one side might be more congested than the opposite side; this is known as the nasal cycle (Fig. 27.2). The nasal cycle is also affected by changes in posture, temperature, humidity, and sleep. The internal valve is defined as the area between the caudal end of the upper lateral cartilages and the cartilaginous septum. The external nasal valve consists primarily of the fibrofatty tissues of the alar lobule and, to a lesser extent, the lower lateral cartilages, the caudal septum, and the piriform aperture. Fig. 27.1 Cartilages of the nose. The upper and lower lateral cartilages are noted along the lateral nasal wall. Note that the medial crura of the lower lateral cartilages extend medially along the caudal septum, where they lie adjacent to the quadrangular cartilage. Fig. 27.2 Nasal cycle. Physiologic congestion, under the control of the autonomic nervous system, causes the nasal mucosa to congest and decongest in a cyclical side-to-side fashion; at any time, one side might be more congested than the opposite side. — Nasal vestibule — Anterior aspect of the inferior turbinate — Anterior nasal septum — Visualization of the midportion or posterior nasal cavity can be challenging. — Provides a detailed and complete examination of the more posterior aspect of the nasal cavity — Middle and superior turbinates and meatus Posterior septum Because ventilation involves pressure changes, the nasal airways must be stable both at rest and under the negative pressures created during quiet and forced inspiration. The internal and external nasal valves depend on satisfactory skeletal stability of the upper and lower lateral cartilages, respectively. When either the skeletal or the soft tissue component is congenitally deficient or has been compromised by surgery or trauma, the patient experiences a dynamic collapse of the valve during inspiration, with resultant airway obstruction. The normal nasal valves collapse with vigorous respiratory effort; however, a patient with dynamic nasal valve dysfunction may have a lateral nasal wall that is so weakened that it collapses even during normal nasal breathing. In most instances, the mucocutaneous and skeletal components and the static and dynamic components contribute in varying degrees to the overall nasal valvular dysfunction. — Static dysfunction is secondary to continuous obstruction at the level of the nasal valve due to deformities such as a deviated septum, inferior turbinate hypertrophy, or inferomedially displaced upper lateral cartilage. — Dynamic dysfunction is obstruction that varies in severity with respiratory effort and is usually related to deficiencies in the structural support of the lateral nasal wall, including the cartilaginous, fibroareolar, and muscular components. The lateral nasal wall caudal to the bony arch is mobile and responds variably to pressure changes.
 Anatomy Pertinent to Nasal Airway Obstruction
Anatomy Pertinent to Nasal Airway Obstruction
 Important Aspects of Assessment Pertinent to Nasal Airway Obstruction
Important Aspects of Assessment Pertinent to Nasal Airway Obstruction
History
 Fixed versus intermittent: early determination of this piece of information provides for a logical initial branching point for development of a differential diagnosis.
Fixed versus intermittent: early determination of this piece of information provides for a logical initial branching point for development of a differential diagnosis.
 Associated factors or complaints
Associated factors or complaints
 Sneezing
Sneezing
 Rhinorrhea
Rhinorrhea
 Epistaxis
Epistaxis
 Headache
Headache
 Nasal pain
Nasal pain
 Past trauma or surgery
Past trauma or surgery
 Exposures
Exposures
 Environmental
Environmental
 Infectious
Infectious
 Medications
Medications
Physical Examination
 Otoscopy
Otoscopy
 Middle ear effusion may indicate pathology in the nose and/or paranasal sinuses or cerebrospinal fluid (CSF).
Middle ear effusion may indicate pathology in the nose and/or paranasal sinuses or cerebrospinal fluid (CSF).
 Negative middle ear pressure (eustachian tube dysfunction): nasopharynx pathology
Negative middle ear pressure (eustachian tube dysfunction): nasopharynx pathology
 Nasal examination
Nasal examination
 Anterior rhinoscopy
Anterior rhinoscopy
 Nasal endoscopy
Nasal endoscopy
 Nasopharyngeal examination
Nasopharyngeal examination
 Indirect technique with mirror; may provide a limited view.
Indirect technique with mirror; may provide a limited view.
 Endoscopic evaluation
Endoscopic evaluation
 Differential Diagnosis of Fixed Obstruction
Differential Diagnosis of Fixed Obstruction
Nasal
 Nasal septal deformity may be the most common source of nasal obstruction. This obstruction is usually unilateral; however, at times it may affect both sides. Patients may have a known history of trauma; occasionally, an insult to the nose may be occult, or the deflection may be developmental in nature. Patients may experience increased sensitivity to the nasal cycle and complain of symptoms that worsen at night. The physical examination often reveals an anterior deflection of the septum with a compensatory hypertrophy of the contralateral or open side. Posterior deflections or septal spurs usually are not as symptomatic as anterior deflections. Septal deviations may also exacerbate or accentuate obstruction in the setting of nasal valve collapse.
Nasal septal deformity may be the most common source of nasal obstruction. This obstruction is usually unilateral; however, at times it may affect both sides. Patients may have a known history of trauma; occasionally, an insult to the nose may be occult, or the deflection may be developmental in nature. Patients may experience increased sensitivity to the nasal cycle and complain of symptoms that worsen at night. The physical examination often reveals an anterior deflection of the septum with a compensatory hypertrophy of the contralateral or open side. Posterior deflections or septal spurs usually are not as symptomatic as anterior deflections. Septal deviations may also exacerbate or accentuate obstruction in the setting of nasal valve collapse.
 Internal nasal valve collapse results from a lack of support to the lateral elements of the nasal vestibule and cavity. It can be divided into mucocutaneous or skeletal/structural disorders. The degree to which lateral wall movement occurs depends on the intrinsic stability of the skeletal and soft tissue support and on the pressure changes the nasal valve is subjected to during quiet and forced inspiration. According to the Bernoulli principle, as the flow velocity of inspired or expired air increases, the pressure inside the nasal vault decreases relative to atmospheric pressure. At a threshold flow velocity, the disparity between pressures inside and outside the nasal vault overcomes the stability of the lateral nasal wall, and collapse occurs. This intrinsic stability derives from the rigidity of the unaltered nasal anatomy or from the support provided by the skeletal and soft tissue elements that remain after rhinoplasty.
Internal nasal valve collapse results from a lack of support to the lateral elements of the nasal vestibule and cavity. It can be divided into mucocutaneous or skeletal/structural disorders. The degree to which lateral wall movement occurs depends on the intrinsic stability of the skeletal and soft tissue support and on the pressure changes the nasal valve is subjected to during quiet and forced inspiration. According to the Bernoulli principle, as the flow velocity of inspired or expired air increases, the pressure inside the nasal vault decreases relative to atmospheric pressure. At a threshold flow velocity, the disparity between pressures inside and outside the nasal vault overcomes the stability of the lateral nasal wall, and collapse occurs. This intrinsic stability derives from the rigidity of the unaltered nasal anatomy or from the support provided by the skeletal and soft tissue elements that remain after rhinoplasty.
 The mucocutaneous component refers to the mucosal swelling (secondary to allergic, vasomotor, or infectious rhinitis) that can significantly decrease the cross-sectional area of the nasal valve and thus reduce nasal airway patency.
The mucocutaneous component refers to the mucosal swelling (secondary to allergic, vasomotor, or infectious rhinitis) that can significantly decrease the cross-sectional area of the nasal valve and thus reduce nasal airway patency.
 The skeletal/structural component refers to any abnormalities in the structures that contribute to the nasal valve area. This includes the nasal septum, upper and lower lateral cartilage, fibroareolar lateral tissue, piriform aperture, head of the inferior turbinate, and floor of the nose. The skeletal component can be further divided into static and dynamic nasal dysfunction.
The skeletal/structural component refers to any abnormalities in the structures that contribute to the nasal valve area. This includes the nasal septum, upper and lower lateral cartilage, fibroareolar lateral tissue, piriform aperture, head of the inferior turbinate, and floor of the nose. The skeletal component can be further divided into static and dynamic nasal dysfunction.
 Nasal fracture as a source of obstruction will be obtained by history. Nasal airway obstruction occurs as a result of decreased cross-sectional area of the nasal cavity due to either soft tissue or nasal skeletal disruption.
Nasal fracture as a source of obstruction will be obtained by history. Nasal airway obstruction occurs as a result of decreased cross-sectional area of the nasal cavity due to either soft tissue or nasal skeletal disruption.
 Septal hematoma/abscess will be responsible for sudden onset nasal obstruction. Patients will usually have an antecedent history of nasal trauma or fracture. Usually, impressive pain accompanies an examination, which demonstrates a pale, purplish, or erythematous fluctuant mass in the anterior portion of the septum. Clinical examination with anterior rhinoscopy or endoscopy may be more beneficial than imaging studies in the diagnosis of this entity.
Septal hematoma/abscess will be responsible for sudden onset nasal obstruction. Patients will usually have an antecedent history of nasal trauma or fracture. Usually, impressive pain accompanies an examination, which demonstrates a pale, purplish, or erythematous fluctuant mass in the anterior portion of the septum. Clinical examination with anterior rhinoscopy or endoscopy may be more beneficial than imaging studies in the diagnosis of this entity.
 Turbinate hypertrophy may be physiologic or pathologic. It is related to an increase in vascular inflow and engorgement of the parenchyma or soft tissue of the inferior turbinates. Rarely, a concha bullosa or air cell in the middle turbinate area will lead to obstruction complaints. Techniques to measure the obstruction objectively may include rhinostereometry or acoustic rhinomanometry; however, most specialists will base the diagnosis on the patient’s history and clinical evaluation.
Turbinate hypertrophy may be physiologic or pathologic. It is related to an increase in vascular inflow and engorgement of the parenchyma or soft tissue of the inferior turbinates. Rarely, a concha bullosa or air cell in the middle turbinate area will lead to obstruction complaints. Techniques to measure the obstruction objectively may include rhinostereometry or acoustic rhinomanometry; however, most specialists will base the diagnosis on the patient’s history and clinical evaluation.
 Nasal polyposis may lead to obstruction, which is unilateral or bilateral. The etiology is related to chronic inflammation of the mucosal lining of the nose and paranasal sinuses. Polyps present as clear or bluish masses of tissue arising from the mucosa of the nasal cavity. There is often some vasculature present on the surface of these structures that is best visualized with an endoscope. Polyposis is often associated with chronic rhinosinusitis, allergic fungal sinusitis, or recurrent acute rhinosinusitis. There is a strong association between polyps and allergic rhinitis, both of which can lead to nasal obstruction. In addition to causing nasal airway obstruction, polyps can be associated with hyposmia or anosmia. Patients with polyposis can also have asthma, allergies, or Samter triad.
Nasal polyposis may lead to obstruction, which is unilateral or bilateral. The etiology is related to chronic inflammation of the mucosal lining of the nose and paranasal sinuses. Polyps present as clear or bluish masses of tissue arising from the mucosa of the nasal cavity. There is often some vasculature present on the surface of these structures that is best visualized with an endoscope. Polyposis is often associated with chronic rhinosinusitis, allergic fungal sinusitis, or recurrent acute rhinosinusitis. There is a strong association between polyps and allergic rhinitis, both of which can lead to nasal obstruction. In addition to causing nasal airway obstruction, polyps can be associated with hyposmia or anosmia. Patients with polyposis can also have asthma, allergies, or Samter triad.
 Bilateral polyps are most common. Occasionally, they are seen on anterior rhinoscopy; however, they are best visualized by endoscopy. Further delineation with radiologic imaging is often warranted.
Bilateral polyps are most common. Occasionally, they are seen on anterior rhinoscopy; however, they are best visualized by endoscopy. Further delineation with radiologic imaging is often warranted.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


