Nasal Fractures
Nasal fractures may occur at any age, but are uncommon in early childhood. They account for the second largest group of facial fractures because of the nose’s prominent position on the face.
37-1 Treatment of Nasal Fractures
Indications
Reduction of nasal fractures is indicated if there is significant cosmetic or functional deformity. Nondisplaced fractures can be managed conservatively with observation and prevention of further injury as the nose heals. Displaced fractures (convex, concave, or comminuted) require reduction under general anesthesia.
Preoperative Evaluation
A complete examination of the nose and surrounding structures is necessary. Associated injuries to the orbit must be identified and treated. Inspection of the nose will usually reveal the nasal deformity. Palpation of the nose may detect bone irregularities (step-offs) on the nasal bones. However, if 30 to 60 minutes have passed, the edema over the bony structures may obscure the deformity.
If the patient is seen several hours after the injury and edema is present, the patient should be reexamined 4 to 7 days later to determine the presence of any nasal deformity after the acute edema has resolved.
Septal hematomas should be detected and treated immediately (see Section 10-1).
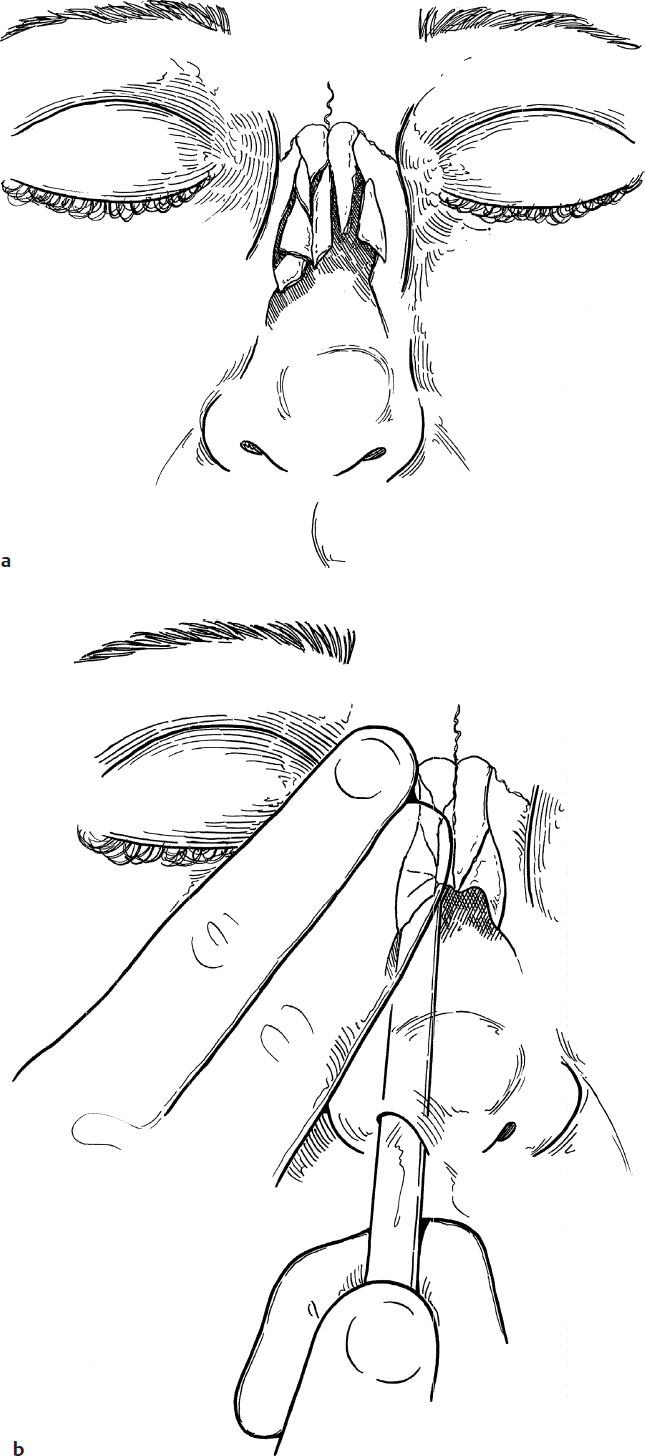
Nasal bone radiographs are occasionally helpful in identifying a fracture site, but only the clinical examination can determine if the cosmetic deformity present is sufficient to justify intervention (Fig. 37.1a).
Nasal fracture reduction is best carried out 4 to 7 days following the injury. This allows tissue edema from the injury to subside and permits a more precise reduction.
Deflection or fracture in the nasal septal cartilage may require further intervention in the future with a septoplasty or septorhinoplasty.
Operative Technique
1. Nasal reduction in children is best accomplished under general anesthesia not only for the comfort of the child but also to protect the airway from bleeding that can ensue intraoperatively.
2. The nose is packed with 4% cocaine hydrochloride using neurosurgical pledgets for decongestion and hemostasis (alternately, any combination of a topical vasoconstrictor and local anesthetic may be used). In younger children, alternates to cocaine should be used.
3. A flat, blunt instrument (e.g., a Boies nasal fracture elevator) is placed external to the nose along its length toward the skull base to approximate a safe insertion depth to avoid skull base injury.
4. The Boies elevator is placed into the nose, and the depressed nasal bone is mobilized anterolaterally (Fig. 37.1b).
5. If the opposite nasal bone is displaced, it is reduced to its normal position manually or with the Boies elevator as described.
6. The fractured fragments are then gently replaced in their normal position by manual palpation (Fig. 37.1c).
7. Care is taken to make sure that the septum is in its normal midline position.
8. Gelfoam (Pfizer) or oxycel (Surgicel [Ethicon]) is then placed in the nose to support the fracture fragments, if necessary. This is rarely needed in young children.
9. An external nasal splint is then placed to prevent reinjury while the nose heals (Fig. 37.1d). This is removed after 5–7 days.
Complications
1. Cosmetic deformity secondary to inadequate reduction
2. Epistaxis
3. Cerebrospinal fluid leak due to aggressive/deep elevator placement