Nasal Deformity
Children frequently sustain nasal trauma from falls or sports. Nasal trauma may cause a deviated septum or displaced nasal bones.
12-1 Conservative Septoplasty
Introduction
Septoplasty should be carefully considered in the pediatric population for risk of disturbing the growth centers in the septum. However, if a child has severe nasal obstruction secondary to septal deviation or recurrent sinus infections as a result of the septal deviation, then a conservative septoplasty may be considered. Removal of a septal spur or minimal resection of cartilage to remove the septal deformity and to improve nasal patency should be the goal of surgery, rather than attempting to achieve a perfectly straight septum.
Indications
Septoplasty may be indicated when there is sufficient septal deformity or deviation to cause nasal obstruction. Septoplasty may also be performed to manage refractory epistaxis.
Preoperative Evaluation
Careful visual inspection of the nasal cavity before and after topical vasoconstriction of the nasal mucosa should be performed. Patients should be evaluated and treated for allergic rhinitis as a potential etiology for nasal congestion/obstruction. Additionally, gastroesophageal reflux may also contribute to posterior nasal mucosal edema and inflammation, contributing to nasal congestion. Radiographic examination is usually not necessary or helpful.
Operative Technique
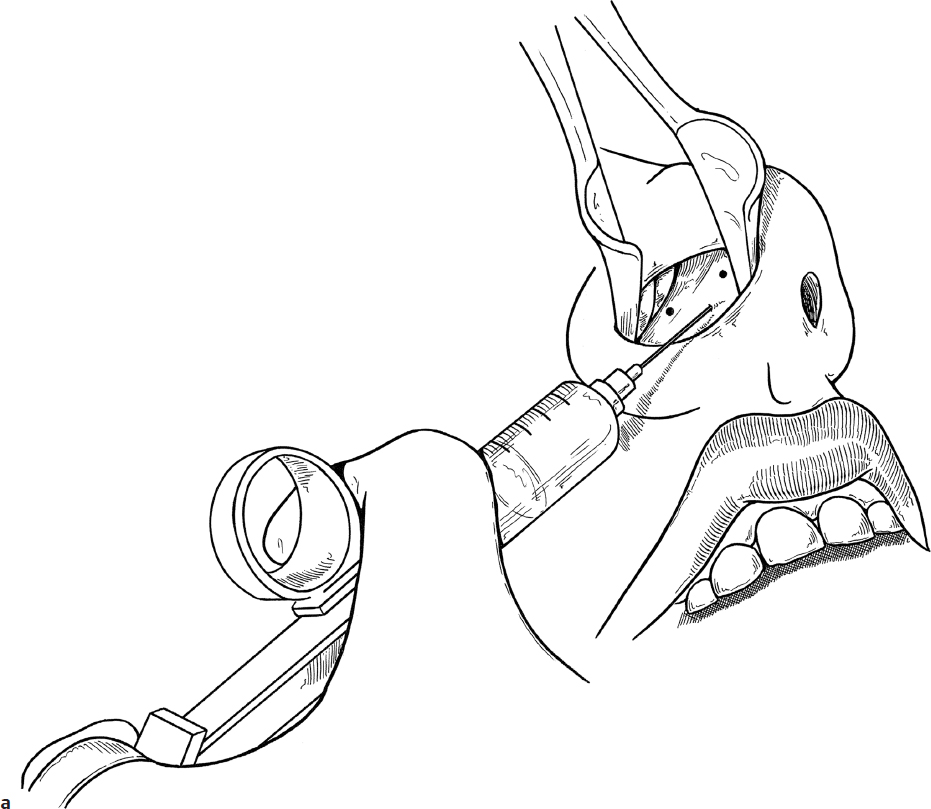
1. General anesthesia is typically required to perform septoplasty in children and teenagers. Additionally, the nasal mucosa is injected with 1% lidocaine with 1:100,000 epinephrine. The injection is placed ideally under the mucoperichondrium to provide hydrodissection and hemostasis (Fig. 12.1a). Additional intranasal decongestion is provided with 4% topical cocaine solution applied with neurosurgical Cottonoid (Codman) pledgets.
2. If there is an isolated septal spur or deformity, a small mucoperichondrial flap may be created directly over the lesion.
a. An incision is made just anterior to the defect through the mucosa and perichondrium, but not through the cartilage (Fig. 12.1b).
b. The mucoperichondrium is elevated off of the spur or deformity (Fig. 12.1c). This can be performed utilizing a headlight or a nasal endoscope. The endoscope may provide better illumination and a magnified view; however, it will limit a surgeon to a single hand to operate or necessitate an assistant to manipulate the scope to allow the surgeon the freedom to use both hands. There are many surgical instruments that have been developed for use in endoscopic surgery; one convenient instrument is a suction elevator.
c. After elevating the flap, the spur or septal deformity can be shaved off using a sharp instrument like a scalpel or Cottle or Freer elevator (Fig. 12.1d).
3. If there is a large deflection or deviation that needs to be addressed, a larger mucoperichondrial flap may be elevated.
a. The mucoperichondrial incision can be made approximately 5 mm cephalad to the caudal edge of the cartilaginous septum. Care is taken not to cut through the cartilage.
b. The mucoperichondrium is elevated using a flat elevator such as a Cottle or Freer elevator or a suction elevator. Once again, this may be performed utilizing a headlight or nasal endoscope.
c. The mucoperichondrial flap is elevated over the septum and, if there is deflection of the bony septum, the mucoperiosteal flap is elevated over the bony septum also.
d. If necessary, a mucoperichondrial flap may be elevated on the contralateral side of the septum by either dissecting around the caudal end of the septum or by making an incision though the cartilage, about 5 mm cephalad to the mucoperichondrial incision, taking care not to cut through the mucoperichondrium on the contralateral side (Fig. 12.1e,f). Care must be taken if dissection is made around the caudal end of the septum so as not to disrupt the support of the nasal tip; otherwise, this will need to be addressed at the time of closure.
e. A small strip of cartilage may be cut or removed to allow for repositioning of the cartilaginous septum. The dorsal and caudal margins of the quadrilateral cartilage need to be preserved to maintain support of the nose (Fig. 12.1g,h).
f. Resection and cutting of the cartilage should be minimized to reduce the potential risk of disturbance of nasal growth.
g. Deviations of the bony septum as well as thick areas and duplications of bone or cartilage may be resected or shaved.
h. Prominent edges of the maxillary crest may also be reduced with a narrow osteotome or ronguer, taking care to avoid cutting through or tearing the overlying mucoperiosteal flap (Fig. 12.1i).
4. Once the deviation/spur/deflection has been addressed, the mucoperichondrial flaps need to be reapproximated to the septum to reduce dead space and to prevent collections between the flaps and the septal cartilage. Various techniques are available to reapproximate the flaps. A simple technique involves using an absorbable suture (e.g., 5-0 Chromic gut [Ethicon]) through and through the septum. There are also endonasal staplers designed to quickly reapproximate the septal flaps (Fig. 12.1j).
5. If a caudal incision was made, it is closed with absorbable suture (e.g., 5-0 Chromic gut).
6. Telfa (Covidien) or Merocel (Medtronic) packs with silk retrieval sutures may be placed on each side of the septum to apply gentle pressure to the septum. These packs may be removed 12–24 hours after surgery. Some surgeons have used reinforced Silastic sheeting (Dow) on each side of the septum to apply pressure and also to reduce the risk of intranasal synechiae (Fig. 12.1k).
Complications
1. Septal perforation
2. Epistaxis
3. Recurrence of septal deviation and persistence of symptoms
4. Saddle nose deformity (loss of dorsal support)
5. Loss of tip projection (loss of tip support from caudal septum)
6. Intranasal synechiae