Laryngotracheal reconstruction can be technically challenging. Successfully managing the patient’s medical comorbidities is essential. Children undergoing laryngotracheal reconstruction rarely present with isolated subglottic stenosis; many have associated multisystem disorders. Effectively managing the patient enables successful outcomes after airway reconstruction.
- •
Laryngotracheal stenosis can be caused or further aggravated by numerous systemic diseases.
- •
A multidisciplinary approach is critical when evaluating and managing children with laryngotracheal stenosis and underlying systemic disease.
- •
Surgical outcomes of laryngotracheal reconstruction can be adversely affected when underlying systemic disease is not properly addressed.
Multisystem disease in the cause of SGS
Pediatric airway reconstruction is performed for congenital or acquired laryngotracheal stenosis. Most SGS is acquired. Infection, autoimmune disease, or massive polytrauma may directly cause acquired SGS or tracheal stenosis with pathologic foci inflicting damage in the airway.
In the early 1900s, the predominant cause for acquired SGS was trauma or infectious diseases such as tuberculosis, syphilis, and diphtheria. With the advent of antibiotics, stenosis resulting from infectious causes significantly decreased.
The practice of long-term intubation in neonates requiring mechanical ventilation was introduced in 1965. This practice led to an increased incidence of SGS. Improved techniques for managing neonatal ventilation have reduced the impact of airway injury caused by intubation. Despite these improvements, the predominant risk factor for SGS remains endotracheal intubation. The endotracheal tube size, length of intubation, tube movement while intubated, traumatic intubation, and presence of infection or gastroesophageal reflux disease (GERD) all contribute to SGS formation in the intubated patient.
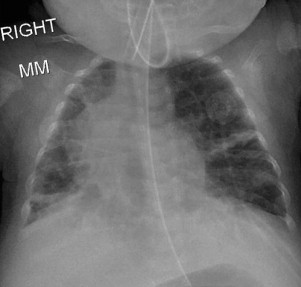
Prematurity is consistently associated with acquired SGS. Treating SGS in the premature neonate presents many unique challenges. Along with a stenotic airway, the premature infant often has compromised lung function with bronchopulmonary dysplasia, neurologic delay, and poor nutrition ( Fig. 1 ).
P earls & P itfalls: The premature patient is the prime example of the challenges encountered in performing LTR in a patient with multisystem disease.
Laryngeal surgery, external neck trauma, burns, or caustic ingestions may also cause SGS. Although rare in the pediatric patient, SGS may develop from systemic autoimmune processes such as Wegener granulomatosis, relapsing polychondritis, and sarcoidosis. Management in these patients initially focuses on treating the underlying disease process. LTR is then considered only after the autoimmune disease is well controlled.
Congenital SGS currently accounts for only 5% of patients with SGS. Congenital SGS occurs in children without any prior intubations or other identifiable cause. The stenosis is attributed to an abnormally shaped cricoid cartilage or incomplete recanalization of the subglottis and is divided histologically into membranous and cartilaginous forms. Children with Down syndrome are at greater risk of congenital SGS. Congenital tracheal stenosis, although rare, is frequently caused by a complete tracheal ring. Tracheal rings are often associated with a pulmonary vascular sling or intracardiac defects.
Multisystem disease in the treatment of SGS
Severe SGS
Treatment options for SGS have increased greatly in the past 40 years. Before the introduction of airway reconstruction in the early 1970s, tracheotomy was the primary long-term treatment of severe SGS. A tracheotomy tube completely bypasses the stenosis, avoiding more potentially invasive treatments of the diseased airway. This option is now most commonly used as a temporizing measure in patients not medically fit for extensive airway reconstruction. Patients with significant cardiopulmonary disease or other comorbidities, who would not tolerate a long general anesthetic, are tracheotomized to provide a secure and stable airway. Diseases known to affect the surgical outcome after laryngotracheoplasty, such as diabetes, upper airway infections, and gastroesophageal reflux, are medically treated and definitive airway reconstruction delayed until these patients are adequately managed.
Mild SGS
Patients with mild stenosis (grade I or mild grade II) may often be observed without any need for surgical intervention. In patients with multisystem disease, decisions regarding management options ultimately necessitate a discussion weighing the risks versus benefits of intervention. Patients with intermittent crouplike symptoms that are exacerbated by upper respiratory tract infections can often be followed conservatively with surveillance endoscopy to ensure that the airway is growing with the child. An active, otherwise healthy child may be more symptomatic with mild-moderate SGS than a neurologically delayed or bed-bound child. Children with limited physical activity and functional abilities may be safer with a tracheotomy or close observation. The goals of any airway reconstruction in these children must be clearly defined by both the caregiver and the surgeon.
Laryngotracheal Stenosis
Laryngotracheal stenosis can be managed through open (transcervical) or endoscopic approaches. Advanced instrumentation and improved techniques have expanded the capabilities of endoscopic interventions in treating SGS in recent years. The endoscopic procedures prevent neck incisions and avoid many of the potential complications associated with open approaches. Balloon dilators, CO 2 lasers, powered microdebriders, and endoscopically placed costochondral grafts have all been used. In the patient with multisystem disease, endoscopic operations provide potentially quicker and less invasive options that may be better tolerated.
Moderate to Severe SGS
Open transcervical approaches are the standard of care in the definitive treatment of moderate to severe SGS. These operations include airway expansion with interpositional cartilage grafts (eg, laryngotracheoplasty with anterior and posterior costochondral grafts) or segmental resection with primary anastomosis (eg, cricotracheal resection). Experienced surgical, anesthesia, and critical care personnel are essential because of the high acuity of these operations. Single-stage laryngotracheoplasty with interpositional cartilage grafts requires stenting via endotracheal intubation for several days. Postoperative pulmonary complications that accompany endotracheal intubation, such as atelectasis, consolidation, and pneumonia, are common. Prophylactic antibiotics are recommended to prevent infections at the site of reconstruction.
P earls & P itfalls: Wound infections in the reconstructed airway can impair healing, destroy grafts, and contribute to the potentially deadly complication of airway dehiscence at the site of reconstruction.
Voice and Swallowing Difficulties
Voice and swallowing difficulties are expected in the immediate perioperative period. Many patients with laryngotracheal stenosis have long-standing voice complaints secondary to prolonged endotracheal tube trauma to the vocal folds. After reconstruction, voice problems are often exacerbated in the expanded airway. Temporary dysphagia and aspiration may occur immediately after surgery but resolve in most cases within a short period of time. Speech language-pathology therapists are helpful in the long-term management of voice and swallowing mechanisms after airway reconstruction.
Multisystem disease in the treatment of SGS
Severe SGS
Treatment options for SGS have increased greatly in the past 40 years. Before the introduction of airway reconstruction in the early 1970s, tracheotomy was the primary long-term treatment of severe SGS. A tracheotomy tube completely bypasses the stenosis, avoiding more potentially invasive treatments of the diseased airway. This option is now most commonly used as a temporizing measure in patients not medically fit for extensive airway reconstruction. Patients with significant cardiopulmonary disease or other comorbidities, who would not tolerate a long general anesthetic, are tracheotomized to provide a secure and stable airway. Diseases known to affect the surgical outcome after laryngotracheoplasty, such as diabetes, upper airway infections, and gastroesophageal reflux, are medically treated and definitive airway reconstruction delayed until these patients are adequately managed.
Mild SGS
Patients with mild stenosis (grade I or mild grade II) may often be observed without any need for surgical intervention. In patients with multisystem disease, decisions regarding management options ultimately necessitate a discussion weighing the risks versus benefits of intervention. Patients with intermittent crouplike symptoms that are exacerbated by upper respiratory tract infections can often be followed conservatively with surveillance endoscopy to ensure that the airway is growing with the child. An active, otherwise healthy child may be more symptomatic with mild-moderate SGS than a neurologically delayed or bed-bound child. Children with limited physical activity and functional abilities may be safer with a tracheotomy or close observation. The goals of any airway reconstruction in these children must be clearly defined by both the caregiver and the surgeon.
Laryngotracheal Stenosis
Laryngotracheal stenosis can be managed through open (transcervical) or endoscopic approaches. Advanced instrumentation and improved techniques have expanded the capabilities of endoscopic interventions in treating SGS in recent years. The endoscopic procedures prevent neck incisions and avoid many of the potential complications associated with open approaches. Balloon dilators, CO 2 lasers, powered microdebriders, and endoscopically placed costochondral grafts have all been used. In the patient with multisystem disease, endoscopic operations provide potentially quicker and less invasive options that may be better tolerated.
Moderate to Severe SGS
Open transcervical approaches are the standard of care in the definitive treatment of moderate to severe SGS. These operations include airway expansion with interpositional cartilage grafts (eg, laryngotracheoplasty with anterior and posterior costochondral grafts) or segmental resection with primary anastomosis (eg, cricotracheal resection). Experienced surgical, anesthesia, and critical care personnel are essential because of the high acuity of these operations. Single-stage laryngotracheoplasty with interpositional cartilage grafts requires stenting via endotracheal intubation for several days. Postoperative pulmonary complications that accompany endotracheal intubation, such as atelectasis, consolidation, and pneumonia, are common. Prophylactic antibiotics are recommended to prevent infections at the site of reconstruction.
P earls & P itfalls: Wound infections in the reconstructed airway can impair healing, destroy grafts, and contribute to the potentially deadly complication of airway dehiscence at the site of reconstruction.
Voice and Swallowing Difficulties
Voice and swallowing difficulties are expected in the immediate perioperative period. Many patients with laryngotracheal stenosis have long-standing voice complaints secondary to prolonged endotracheal tube trauma to the vocal folds. After reconstruction, voice problems are often exacerbated in the expanded airway. Temporary dysphagia and aspiration may occur immediately after surgery but resolve in most cases within a short period of time. Speech language-pathology therapists are helpful in the long-term management of voice and swallowing mechanisms after airway reconstruction.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


