Purpose
To examine movement of the internal canalicular orifice with blinking and lacrimal drainage under endonasal endoscopic observation after dacryocystorhinostomy.
Design
Observational anatomic study.
Methods
Twenty internal canalicular orifices (right 9, left 11) from 15 patients (age range: 44-77 years) who underwent endoscopic endonasal dacryocystorhinostomy were prospectively examined. The patients sat on a chair with the chin projected slightly upward while digital images were taken. After examining the movement of the internal canalicular orifice with blinking, the patient’s eye was stained with fluorescein dye, and diffusion from the orifice was examined with blinking.
Results
The internal canalicular orifice closed during eyelid opening, although always incompletely. In eyelid closing, the orifice opened, and was pulled laterally without folds. All 20 internal canalicular orifices formed a diverticulum. Three specimens illustrated the upper and lower canalicular ends emptying into the diverticulum. The closing of these canalicular ends was always incomplete. Movement of the internal canalicular orifice was slight during normal blinking, but forced blinking resulted in more movement. Movement of the lacrimal sac wall was slight. During the first few seconds without blinking, no fluorescein dye flowed from the orifice. After several blinks, fluorescein dye flowed out slowly from the orifice, and increased in volume with more blinking. The fluorescein dye traveled inferiorly by gravity. A forced blinking was related to more dye inflow.
Conclusions
The internal canalicular orifice incompletely closed during eyelid opening, but this orifice largely opened during eyelid closing, with a slow gravitational inflow of lacrimal fluid.
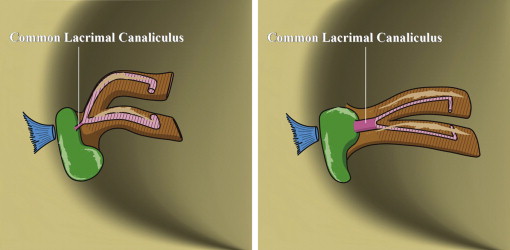
Movement of the internal canalicular orifice is one of the key factors in lacrimal drainage. Based on the anatomy, we previously speculated a common canalicular movement with blinking, and a functional valve mechanism at this site. During eyelid opening, the Horner muscle relaxes and pushes the common lacrimal canaliculus, leading to its occlusion ( Figure 1 ). In contrast, during eyelid closing, the Horner muscle contracts and moves away from the common lacrimal canaliculus, inducing its dilation ( Figure 1 ). In addition to this mechanism, additional functions such as gravity, pressure gradients in the lacrimal tract, and tear reabsorption by the cavernous structure support the lacrimal drainage.
The purpose of the present study was to examine movement of the internal canalicular orifice with blinking and lacrimal drainage at this site under endonasal endoscopic observation after dacryocystorhinostomy (DCR).
Methods
Twenty internal canalicular orifice areas (right 9, left 11) from 15 patients who underwent endoscopic endonasal DCR were studied in this prospective cross-sectional study to examine movement of this area in association with blinking. This study was performed about 1 month postoperatively using a rigid nasal endoscope of 4 mm diameter with a 70-degree tip (EN-6570; MACHIDA, Tokyo, Japan) introduced into the DCR ostium after 10 minutes of gauze packing soaked with epinephrine (1:5000 solution) in the nasal cavity for mucosal shrinkage. This study was approved by the institutional review board of Aichi Medical University (no. 12-141), with the appropriate informed consent obtained from all patients, and adhered to the tenets of the Declaration of Helsinki.
The video recording was performed by a single examiner (H.K.) with a digital camera (G700; RICOH, Tokyo, Japan). The endoscope was connected to the digital camera with a C-mount (CAE-1; MACHIDA). All DCR were performed by a single surgeon (H.K.) with an endoscopic endonasal technique, using mitomycin C, under general anesthesia, because endoscopic endonasal DCR preserves the pump mechanism of the orbicularis oculi muscle.
The patient sat on a chair with the chin projected at a slight anterior angle. After examination of the movement of the internal canalicular orifice with blinking, the patient’s eye was stained with fluorescein dye, and diffusion from the internal canalicular orifice in association with blinking was measured.
Although some of the upper and lower canaliculi are known to separately reach the lacrimal sac without forming a common canaliculus, we defined the canaliculus just before entering the sac as the “common lacrimal canaliculus” and its exit to the sac as the “internal canalicular orifice.”
Results
The average age of patients was 65.5 years (range: 44-77 years). The internal canalicular orifice closed during eyelid opening, but this closing was always incomplete ( Figure 2 ). This was shown in all 20 orifices. During eyelid closing, the internal canalicular orifice opened completely and was pulled deeply in a lateral manner, with no folds or membranes shown ( Figure 2 ). All 20 internal canalicular orifices formed a diverticulum, referred to as the sinus of Maier. This observation was especially obvious when the eyelid was closed.
Three specimens illustrated simultaneously the upper and lower canalicular ends, but these also emptied into the diverticulum ( Figure 2 and Supplemental Video 1 , available at AJO.com ). The closing of these canalicular ends was also always incomplete ( Supplemental Video 1 ). The movement of the internal canalicular orifices was slight during normal blinking, but forced blinking caused the internal canalicular orifices to move to a greater extent ( Supplemental Video 1 ). Movement of the lacrimal sac wall was slight ( Supplemental Video 1 ).
Diffusion of the fluorescein dye from the internal canalicular orifice can be illustrated in association with blinking ( Figure 3 and Supplemental Video 2 , available at AJO.com ). Within the first few seconds without blinking, no fluorescein dye flowed in from the internal canalicular orifice, which was found in all 20 orifices. After several eyelid blinks, the fluorescein dye diffused from the internal canalicular orifice, and it increased in volume with more blinking. The fluorescein dye moved inferiorly according to gravity. Forced blinking correlated with more inflow of the dye in all 20 cases.
Results
The average age of patients was 65.5 years (range: 44-77 years). The internal canalicular orifice closed during eyelid opening, but this closing was always incomplete ( Figure 2 ). This was shown in all 20 orifices. During eyelid closing, the internal canalicular orifice opened completely and was pulled deeply in a lateral manner, with no folds or membranes shown ( Figure 2 ). All 20 internal canalicular orifices formed a diverticulum, referred to as the sinus of Maier. This observation was especially obvious when the eyelid was closed.



