Purpose
To report the results of simple limbal epithelial transplantation using a double-layered cryopreserved amniotic membrane graft for the management of unilateral limbal stem cell deficiency.
Design
Retrospective case series.
Methods
Four consecutive patients with unilateral partial (2 eyes) and total (2 eyes) limbal stem cell deficiency secondary to ocular surface burns (2 eyes), trauma (1 eye) and conjunctival melanoma treatment (1 eye) underwent modified simple limbal epithelial transplantation at Bascom Palmer Eye Institute. Preoperative and postoperative visual acuity and quality of corneal epithelium were evaluated.
Results
The patients were followed up for a mean ± standard deviation of 7.5 ± 1.3 months. The donor eye returned to a healthy state in all patients. All patients had significant improvement in visual acuity and resolution of ocular pain in the affected eye. Regular corneal epithelium and a quiet ocular surface were obtained in all patients by a median of 4 weeks.
Conclusions
Compared with the currently used surgical techniques for management of limbal stem cell deficiency, simple limbal epithelial transplantation seems to be a safe, reproducible, and effective alternative. The use of a double layer allows more protection for the explant without impacting outcomes. Also, the use of cryopreserved amniotic membrane allows surgeons to perform this procedure in the Unites States. More cases with longer follow-up will be needed to assess the outcomes further.
Limbal stem cell deficiency is a common phenotypic end point of various ocular pathologic features, the most common of which are severe inflammatory insults to the ocular surface such as chemical or thermal burns. Other causes include immunologically induced inflammation such as Stevens-Johnson syndrome and ocular cicatricial pemphigoid, along with mechanical, infectious, iatrogenic, idiopathic, and hereditary causes. As limbal stem cells fail to generate and maintain basal cells for the corneal epithelium, conjunctival epithelium starts invading the superficial cornea. Patients usually have pain and photophobia secondary to recurrent corneal erosions. Superficial neovascularization and conjunctivalization also emerge and eventually lead to visual impairment. Visual rehabilitation is difficult in these patients because corneal transplantations almost universally fail.
Efforts have been made to reinstate a healthy ocular surface with limbal stem cell transplantation. However, limitations in the available techniques have limited its widespread use. Traditional conjunctival limbal autografts harvested from the nonaffected eye are limited by the degree of limbal stem cell deficiency in the affected eye and the risk of destabilizing the ocular surface in the good eye. Keratolimbal allografts usually are reserved for bilateral limbal stem cell deficiency, given the need for systemic immunosuppression or otherwise guarded long-term success. Outcomes after autologous ex vivo cultivated limbal epithelial transplantation have been promising with faster epithelialization, less inflammation, and less scarring than traditional autograft. This technique, however, is limited by the high cost and the need for a good manufacturing practice facility to process and expand the cells properly. Currently in the United States, there is no Food and Drug Administration approval for using this type of facility to expand limbal stem cells ex vivo from the healthy eye of a patient and then transplant them back to the patient’s affected eye.
Recently, Sangwan and associates have introduced simple limbal epithelial transplantation, a novel approach that avoids the drawbacks of the existing techniques. In his technique, a small (2 × 2-mm) donor limbal graft from the unaffected eye is harvested and divided into smaller pieces that are then expanded in vivo in the stem cell-deficient eye with the use of a fresh amniotic membrane and fibrin glue. Herein we describe our modification where 2 amniotic membrane layers are used to sandwich and protect the harvested limbal stem cells. Using this technique, we demonstrate the safety and efficacy of using cryopreserved amniotic membrane grafts, a Food and Drug Administration-approved alternative in the United States.
Methods
This study was a retrospective case series of 4 consecutive patients. Through it, we present our experience at Bascom Palmer Eye Institute and the Miami Veterans Affairs Hospital using the simple limbal epithelial transplantation technique to manage unilateral partial or complete limbal stem cell deficiency.
The study was conducted in accordance with the tenets of the Declaration of Helsinki, federal and Florida laws, and the Health Insurance Portability and Accountability Act. This study was exempted from approval by the University of Miami and Miami Veterans Affairs Hospital Institutional Review Boards because it was considered nongeneralizable human research by each.
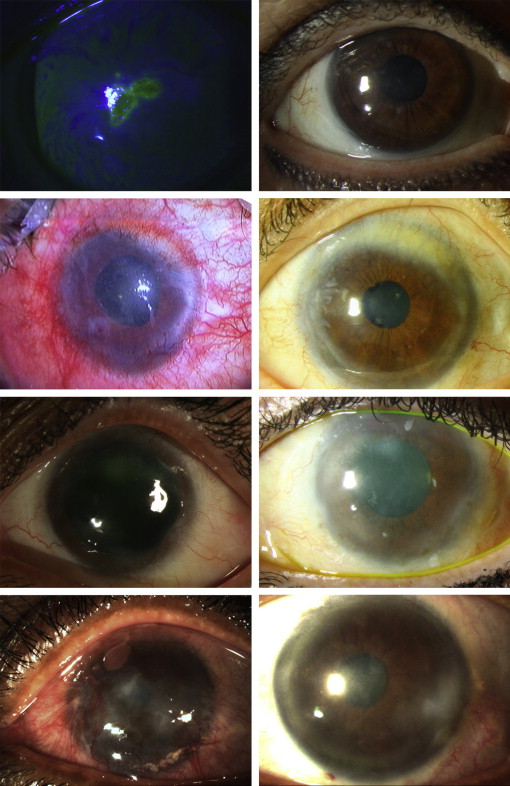
The diagnosis of limbal stem cell deficiency was made clinically by confirming in the affected eye an irregular corneal epithelium, superficial corneal vascularization, persistent epithelial defects, and, in the cases of total limbal stem cell deficiency, a complete conjunctivalization of the cornea ( Figure 1 , Left). Posterior segment evaluation was carried out by ultrasound biomicroscopy in patients where visualization was not possible. Three surgeries were performed by one author (G.A.), and 1 surgery was performed by another author (A.G.). We followed the technique described by Sangwan and associates. The original technique describes the use of fresh amniotic membrane. This option is not available in the United States; instead, we used cryopreserved amniotic membrane (AmnioGraft size B; Biotissue, Inc., Miami, Florida, USA). In brief, and similar to what was described in their article, a 2 × 2-mm area was marked across the supranasal limbus of the donor eye. A subconjunctival dissection was carried out 1 mm into the clear cornea to excise the limbal tissue. The donor tissue then was placed in balanced salt solution. In the affected eye, a 360-degree conjunctival peritomy was performed and the fibrovascular pannus was excised. Bleeding was controlled by gentle cauterization, and the corneal and limbal surface was polished with a diamond bur. An amniotic membrane graft was placed stroma side down on the bare ocular surface and was secured with fibrin glue (Tisseel; Baxter, Deerfield, Illinois, USA). The donor limbal tissue was cut into approximately 12 to 15 pieces with Vannas scissors and placed on the amniotic membrane overlying the cornea in a spiral fashion, sparing the visual axis. The tissue then was secured with fibrin glue. We then modified the original simple limbal epithelial transplantation technique by placing the harvested tissue between the 2 layers of amniotic membrane with the intention of replicating a fetal environment for the stem cells. The second amniotic membrane graft was sutured with 10-0 nylon in a purse string fashion around the limbal area, and then a bandage contact lens (18-mm Kontur lens; Kontur Contact Lens, Co., Inc., California, USA) was placed. All patients were administered topical broad-spectrum antibiotics until the contact lens was removed and prednisolone acetate 1% for 4 to 6 weeks. The bandage contact lens was removed 10 to 14 days after surgery, and the nylon suture was removed after the membrane dissolved. Clinical examination was performed at 1 day then 1 week then 1, 3, and 4 months after surgery, then at 2- to 3-month intervals. Clinical examination by biomicroscopy was documented.
Results
Demographics and clinical details of the 4 patients are provided in the Table . Two females and 2 males were included with a mean age ± standard deviation of 59.8 ± 10.9 years. Duration of limbal stem cell deficiency varied between 3 and 45 years, with a median of 15.5 years. Two eyes of 2 patients had partial unilateral limbal stem cell deficiency secondary to chemical injury (1 eye) and trauma (1 eye), and 2 eyes had total unilateral limbal stem cell deficiency secondary to chemical injury (1 eye) and conjunctival melanoma treatment (1 eye). All patients reported symptoms before surgery, including ocular pain, photophobia, and foreign body sensation. Corneal findings included chronic or recurrent epithelial defects (4 eyes), corneal neovascularization and partial corneal conjunctivalization (2 eyes), complete corneal conjunctivalization (2 eyes), stromal scarring (3 eyes), and pyogenic granuloma formation (1 eye). All patients had bilateral wet ocular surface.
| Patient No. | Age (y) | Sex | Eye | Limbal Stem Cell Deficiency Cause (Time; y) | Limbal Stem Cell Deficiency Degree | Preoperative Treatment | Preoperative Best-Corrected Visual Acuity | Follow-Up (mos) | Stabilization of Ocular Surface (wks) | Postoperative Best-Corrected Visual Acuity |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 74 | Female | Right | Melanoma excision + mitomycin C (3) | Total | Excisional biopsy, cryotherapy, intraoperative and postoperative mitomycin C, cataract extraction with intraocular lens placement | 20/400 | 9 | Yes (2) | 20/40 |
| 2 | 57 | Male | Right | Chemical (ammonium) injury (45) | Total | Ocular restoration with amniotic membrane graft | 20/200 | 7 | Yes (3) | 20/30 |
| 3 | 48 | Female | Left | Chemical injury (16) | Partial | Ocular restoration with amniotic membrane graft | Counting fingers at 1 m | 8 | Yes (1) | 20/50 |
| 4 | 55 | Male | Left | Mechanical trauma (15) | Partial | Ocular restoration with amniotic membrane graft | Counting fingers at 1 m | 6 | Yes (3) | 20/50 |
There were no intraoperative or postoperative complications in any of the 4 cases. After surgery, the donor eye in all patients returned to its healthy state by the first week ( Figure 2 , Left), whereas in the grafted eye, the amniotic membrane sandwich was seen in all patients ( Figure 2 , Right). On slit-lamp examination, the amniotic membranes were no longer visible after a median of 4 weeks, and the cornea had a stable epithelium with a quiet ocular surface. Ultra–high-resolution optical coherence tomography performed at 4 months after surgery for Patient 1 showed a normalized corneal epithelium and a hyperreflective subepithelial layer, likely the residual amniotic membrane graft in the recipient eye ( Figure 3 ). A stable surface with no evidence of epithelial defects or conjunctivalization was maintained in all recipient eyes at a mean ± standard deviation follow-up of 7.5 ± 1.3 months ( Figure 1 ). In all 4 patients, residual islets of tissue in the paracentral cornea were observed after surgery. Explants initially were thick and thinned out over a period of 3 months such that they were barely visible. Best-corrected visual acuity improved from worse than 20/200 in all recipient eyes before surgery to 20/50 or better in all 4 patients ( Table ). After surgery, all patients had complete resolution of pre-existing ocular symptoms including pain, tearing, and photophobia.



