Midface Fractures
Midface fractures are rare in children for a variety of reasons. In children, the midface occupies a relatively small portion of the head and is relatively small and flat as compared to the more prominent cranium. Also, the poorly developed paranasal sinuses result in crush or greenstick injuries rather than complete fractures. Additionally, pediatric bones are more elastic as compared to adult bones. Facial fat pads can provide additional protection to the underlying facial skeleton.
41-1 Treatment of Midface Fractures
Indications
A mobile/depressed midface requires open surgical treatment. Observation can be employed with nondisplaced fractures.
Preoperative Evaluation
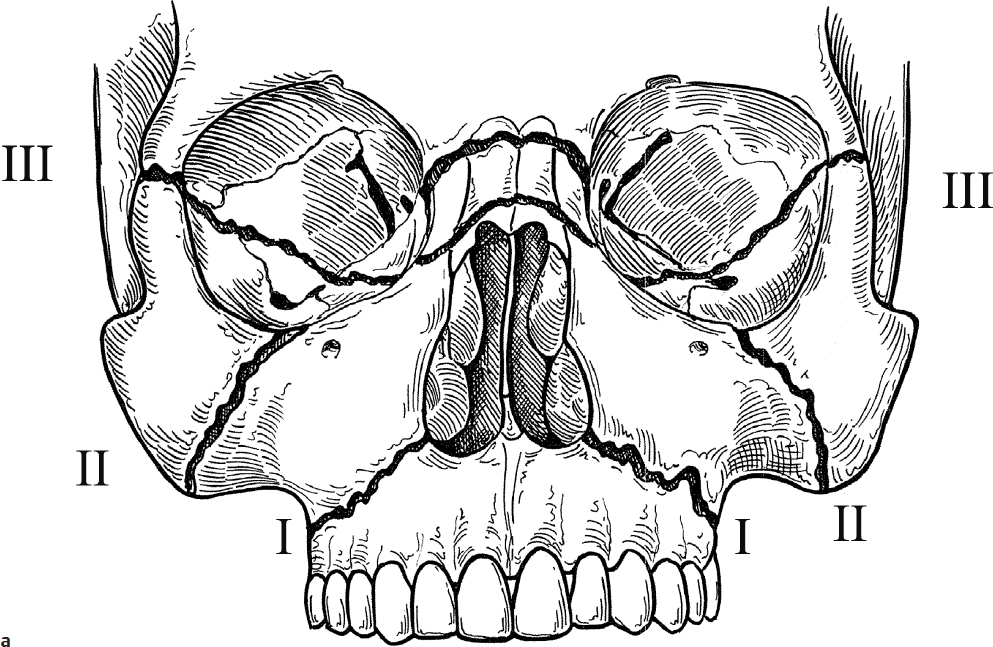
Pediatric low-dose radiation computed tomography (CT) of the facial bones is the best study to define the fractures. Because the injuries are usually the result of severe trauma, associated injuries must be suspected. The airway may also be compromised. The injury is categorized by the location of the fracture: Le Fort I, II, or III (Fig. 41.1a,b). Location of the fracture is important to determine the stable site on the facial skeleton that is to be used for fixation and immobilization. The principles of management include restoration of midface projection and normal maxillomandibular occlusion. Additionally, vertical maxillary buttresses (anterior maxillary buttress, zygomaticomaxillary buttress, and pterygomaxillary buttress) need to be reestablished/stabilized.
These fractures are usually treated more conservatively than in adult patients. Intervention needs to be prompt in the pediatric population due to accelerated bone healing and greater osteogenic potential—preferably between 2 and 4 days after injury.
Minimally displaced fractures and most greenstick fractures without malocclusion can be treated conservatively with liquid to soft diet, restriction of activity, and analgesics. Minimally displaced fractures occurring during the period of tooth development require no treatment or brief maxillomandibular fixation (MMF). However, open reduction is indicated for severely/unstable displaced fractures, occlusal involvement, and orbital involvement.
Operative Technique
Maxillomandibular Fixation and Closed Reduction
1. Midface fractures are best reduced utilizing general anesthesia.
2. Arch bars or Ivy loops can be placed for MMF. Ivy loops are suggested by some for younger children with primary or mixed dentition. Some advocate for arch bars in only older kids with permanent dentition (> 11 years old). Please see Section 42-1 for details of placement of Ivy loops/arch bars.
3. The attachment of the suspension wire to the teeth can be accomplished utilizing an arch bar, bonded hooks, wire loops, or a dental plate. Assistance from a dentist or orthodontist can be very helpful in this step.
4. For children with minimally displaced fractures managed by closed reduction, a short 2–3 week period of MMF with elastics is usually sufficient.
5. MMF is released 2–3 weeks after reduction to prevent temporomandibular joint ankylosis.
Open Reduction and Internal Fixation
1. Midface fractures are best reduced utilizing general anesthesia.
2. The patient is first placed into MMF to restore original occlusion.
3. Direct exposure of all fractures is required. Zygomaticofrontal process fractures can be exposed using an upper blepharoplasty or lateral eyebrow incision (see Section 39-1). Zygomaticomaxillary fractures can be exposed using a subciliary or transconjunctival incision (see Section 39-1). Le Fort I fractures can be exposed through a sublabial incision, with careful attention paid to identify and preserve the infraorbital nerve as it exists its foramina (see Section 38-1).
4. Reduction and alignment of fractures is performed.
5. Internal fixation is performed using 1.5- or 2.0-mm resorbable miniplates and monocortical screws (Fig. 41.1c). Some centers use titanium plates. Some advocate for removal of the titanium plates after 2–3 months in children under 10 years old; however, this is a controversial topic (see Section 39-1). Unerupted tooth buds in children under 6 years of age should be preserved in the placement of screws on the maxilla.
Complications
1. Persistent diplopia
2. Persistent enophthalmos
3. Infection
4. Hardware failure
5. Malunion/nonunion
6. Injury to unerupted teeth
7. Dental malocclusion