, Vincent Y. W. Lin2 and Joseph M. Chen2
(1)
Department of Otorhinolaryngology, Medical University of Vienna, Vienna, Austria
(2)
Department of Otolaryngology Head & Neck Surgery, Sunnybrook Health Sciences Center, Toronto, Ontario, Canada
The most common indications for this approach are repair of superior semicircular canal dehiscence and approach to the IAC for acoustic neuroma resections. Usually small, intracanalicular tumors with good hearing are approached via this route. Vestibular nerve section and total facial nerve decompression, CSF leak, and meningocele repair are other less common indications for this approach. There is significant temporal lobe retraction during this approach, so this makes it less suitable for older patients.
For the middle fossa approach, the surgeon sits at the head of the table, the patient is in supine position, and the head is rotated to the contralateral side. A skin incision starting anterior to the tragus (preauricular crease) and extending superiorly to the parietal suture in a straight line or lazy-S configuration is performed (Fig. 13.1).
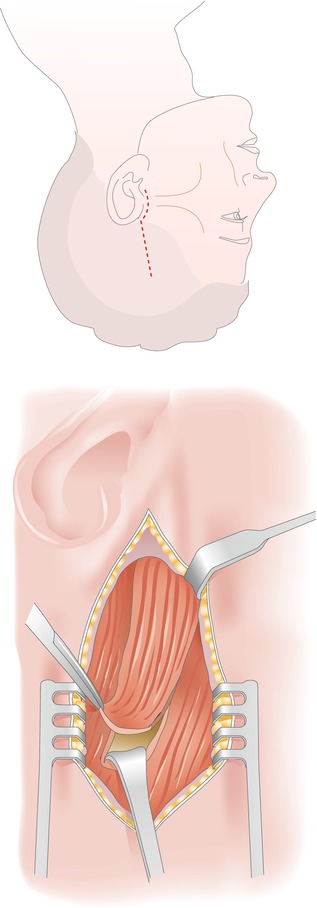
Fig. 13.1
A skin incision from the preauricular crease to the parietal suture is performed. The temporalis muscle is incised and retracted
The temporalis muscle can be incised to create a rotational flap permitting its use for subcranial reconstruction as shown in Fig. 13.1. Alternatively, a vertical linear incision can be made and retracted to expose the skull directly below. An approximately 4 × 6-cm (or larger) craniotomy is performed.
 The craniotomy should be positioned as low as possible to maximize exposure of the middle fossa floor. Sometimes it is necessary to drill the inferior bony margin of the craniotomy to reach the floor (Fig. 13.2).
The craniotomy should be positioned as low as possible to maximize exposure of the middle fossa floor. Sometimes it is necessary to drill the inferior bony margin of the craniotomy to reach the floor (Fig. 13.2).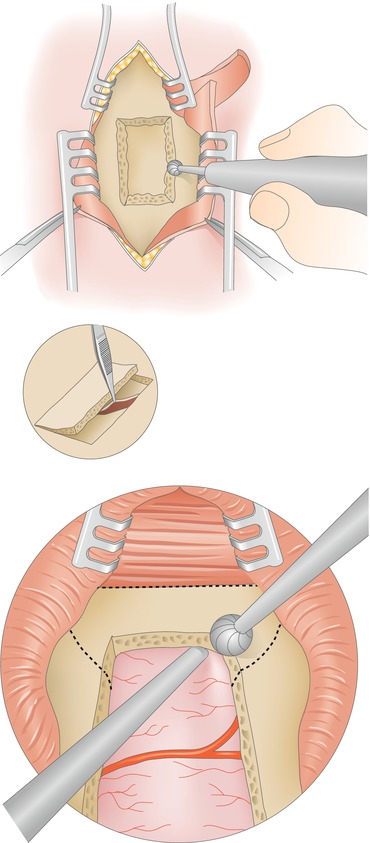
Fig. 13.2
A craniotomy of 4 × 6 cm is performed with the use of an otologic drill or a craniotome. Care is taken not to perforate the dura. The inferior margin of the craniotomy is drilled down to be flush with the floor of the middle fossa (right side, dashed line)
If the temproal bone is well pneumatized and air cells are exposed during this apporach they must be obliterated with bone wax at the end of the case to minimize the risk of a post-operative cerebrospinal fluid leak.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


