23 Meniere Disease
Meniere disease is defined by a group of symptoms including fluctuating sensorineural hearing loss, episodic vertigo, tinnitus, and aural fullness. The disease process is quite variable in severity, progression, manifestations, bilaterality, and response to treatments. Consequently, our understanding of the underlying pathophysiology and efficacy of various treatment options remain controversial. The presumed pathophysiology is endolymphatic hydrops affecting both the cochlea and labyrinth. Although, even this basic presumption has been called under question, the epidemiology, pathophysiology, clinical presentation, and treatment options will be reviewed.
Historical Perspective
French physician Prospere Meniere first described the disease in 1861 in a study presented to the French Academy of Medicine.1 He described the case of a young man with recurrent attacks of vertigo that were followed by the perception of loud noises along with decreased hearing. This study was the first to describe the constellation of these symptoms as a single disease entity. Dr. Meniere’s paper also proposed the revolutionary and somewhat controversial theory that vertigo could result from damage to the inner ear. At that time, the inner ear was known to be responsible for hearing, but its role in balance and equilibrium had not yet been identified. In the mid-19th century, vertigo was thought to be caused by “apoplectiform cerebral congestion,” a broad term indicating overfilling of the brain’s blood vessels. Although Meniere actually proposed that this symptom constellation was caused by hemorrhage into the labyrinth rather than endolymphatic hydrops, the disease has since borne his name.
Epidemiology
Prevalence
There is a wide range of reports on Meniere disease prevalence in the literature. This is likely because of both a variance in presentation and difficulty in diagnosis.
Harris and Alexander examined a large health claims database, comprising over 60 million insured patients from 97 health plans, to estimate the number of patients who carried an International Classiffication of Diseases-9 coded diagnosis of Meniere disease. They concluded there to be an estimated prevalence of 190 per 100,000.2
The most often cited study regarding Meniere disease prevalence is Waserman et al, which demonstrated a prevalence of 218 per 100,000.3 The current diagnosis guidelines for Meniere disease were not established at that time, and one-third of their patients had recurrent vertigo without cochlear symptoms. Thus, their estimate is likely high.
Radke et al4 found a prevalence of 120 per 100,000 by a random survey of 4869 people in Germany. Patients were first screened for moderate to severe vertigo. Then further questions were asked via telephonic interview using the 1995 American Academy of Otolaryngology Committee on Hearing and Equilibrium (CHE) diagnostic criteria.
Age
As expected for a chronic, nonlethal disease, prevalence increases within the population with age. In the study by Harris and Alexander, there were 9 cases per 100,000 of Meniere disease in patients less than 18 but to 440 per 100,000 in patients 65 and older. Age of onset is thought to be most common from age 40 to 50.5
Gender
As with overall prevalence, the gender preponderance was varied across studies, ranging from a slight male predominance6 to 4.3:1 female to male ratio.7 In the study by Harris and Alexander, female preponderance was found to be 1.89:1, which was statistically significant.2
Inheritance
Sporadic versus Familial
Most cases of Meniere disease are sporadic. A small percentage of cases, however, appear to be familial. Various studies have demonstrated a range of 2.6 to 12% of familial cases of total Meniere cases, with an average reported to be 7%.
Although the exact genetic mutations are yet unknown, the inheritance pattern of familial Meniere disease is thought to be autosomal dominant with an incomplete penetrance.5 The penetrance is estimated to be approximately 60%.
An association with human leukocyte antigen (HLA) type has also been proposed. It is thought that some major histocompatibility complexes are more susceptible to Meniere disease than others. HLA type CW7 was found to be associated with a higher incidence of Meniere.8 Additional HLA types found to be associated are A3, B7, and DR2 in other studies.9,10
Pathophysiology
The presence of endolymphatic hydrops has been the central histologic feature of Meniere disease, although the exact pathophysiologic mechanisms are largely unknown. In 1938, Halpike and Cairns reported the histologic description of endolymphatic hydrops in two patients who died postoperatively following vestibular neurectomies for their Meniere disease.11 Independently, in the same year Yamakawa reported the same histopathologic findings.12
Revisiting this topic in 2005, Merchant et al examined 107 temporal bone specimens with and without Meniere disease. Histologic endolymphatic hydrops (Fig. 23.1) was observed in all 28 specimens of patients with known Meniere disease. However, hydrops was also seen in 19 bones from patients without Meniere disease.13 This calls into question the accepted belief that endolymphatic hydrops is the cause of symptoms in Meniere disease; hydrops may rather be an epiphenomenon resulting from underlying cochlear pathology.
Anatomic, infectious, immunologic, and allergic mechanisms have all been proposed to be the initial origin of the disease, but no studies have convincingly proven any of these to be the inciting factor in this disease. Further investigations must be performed that revisit the underlying pathophysiologic mechanisms of this disease.
A recent study by Chiarella et al14 examined the protein content found in blood plasma of Meniere patients compared with healthy controls. They found that certain proteins were found in different concentrations between the two groups. Specifically, complement factor H and B, fibrinogen α and gamma chains, β-actin and pigment epithelium derived factor are overexpressed; on the other hand, the levels of β-2 glycoprotein-1, vitamin D binding protein and apolipoprotein-1 are significantly decreased in the plasma of Meniere disease patients. Although the clinical significance is yet unclear, the biochemical profile may assist in diagnostic tests in the future.
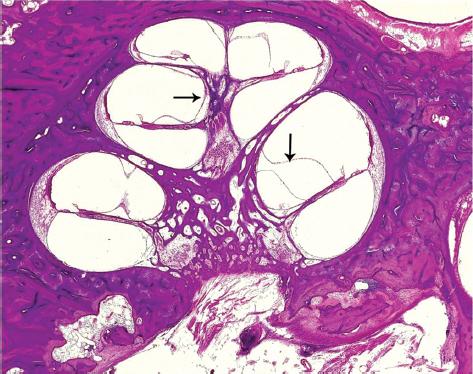
Figure 23.1 Histologic specimen demonstrating endolymphatic hydrops (arrows indicate dilated scala media).
Image Courtesy of Jose Fayad, House Ear Institute.
The role of autoimmunity in the pathophysiology of Meniere disease remains controversial. One line of evidence in support of an autoimmune etiology is the increased incidence of other autoimmune diseases in sporadic Meniere disease patients. Morrison et al reported an incidence of concurrent autoimmune disease in 10.3% of Meniere patients compared with 4% incidence in controls.15 They found similar associations in familial Meniere disease. Ruckenstein et al demonstrated no serologic evidence of autoimmune disease in unilateral Meniere’s aside from a higher incidence of antiphospholipid antibodies but did note an increased incidence of elevated antinuclear antibody (ANA) titers in bilateral Meniere.16
Clinical Presentation
Meniere disease manifests quite variably with regard to the severity, duration of attacks, and natural course. Severe vertigo is often the first, and most debilitating symptom for the Meniere patient. The duration of these acute episodes typically range from minutes to 2 to 3 hours. Nausea and vomiting may accompany the vertigo, and even after the true spinning vertigo resolves, disequilibrium and nondescript dizziness can persist for up to a couple of days after the attack has subsided. Other diagnoses should be entertained in patients in whom the vertigo persists for more than several hours or the residual symptoms persist for more than 24 to 48 hours.
One of the hallmarks of the disease is the presence of fluctuating and progressive hearing loss. Patients most often present with an up-sloping, low-frequency sensorineural hearing loss that, over time, progresses to a more severe, flat sensorineural loss. Hearing loss typically stabilizes about 5 years after disease onset. In a retrospective study of 161 patients with long-term follow-up (9 years), Stahle et al found a mean hearing loss of 50 dB in low and high frequencies.17
An important characteristic of Meniere disease is the temporal relationship between the episodic vertigo, fluctuating hearing loss, tinnitus, and aural pressure sensation. Although the relationship of these symptoms may vary, the characteristic presentation is that the symptoms are temporally related. The typical presentation is that the aural pressure increases concomitant with a reduction in hearing, an increase in tinnitus, and the onset of the vertigo.
Other variations include Lermoyez variant in which the patient experiences aural pressure and hearing loss followed by an improvement in the hearing concomitant with the onset of spinning vertigo. Another variation is the otolithic crisis of Tumarkin. These drop attacks, are a dangerous variant presentation of Meniere disease.18 When Tumarkin first described these attacks, he attributed these events to acute utriculosaccular dysfunction. It is thought that an abrupt change in otolithic input generates an erroneous vertical gravity reference. This in turn generates an inappropriate postural adjustment by way of the vestibulospinal pathway, resulting in a sudden fall. The patient will describe the sensation of being violently pushed downward to the floor. These episodes present quite acutely, often without any warning. The role of the utricle and saccule has been further supported by vestibular-evoked myogenic potentials testing in these patients.19
There is some controversy over the diagnosis of Meniere in patients with only vestibular or cochlear manifestations. It has not been established whether these variations are in the continuum of the disorder or whether they are independent disease processes. Almost 80% of patients who present with episodes of vertigo in the absence of hearing loss and diagnosed with vestibular hydrops or “vestibular Meniere” go on to develop classic Meniere. Whereas only 20% of patients diagnosed with cochlear hydrops or “cochlear Meniere” will proceed to classic Meniere.20
The high incidence of progression from vestibular involvement alone to classic Meniere would argue that vestibular hydrops is a variant of Meniere. Whereas, the low progression from cochlear hydrops to classic disease might suggest that a second pathophysiology is involved.
Physical Examination
Patients with Meniere disease will typically have a normal physical examination unless they are seen during an acute attack. During an acute attack, the patient will often be nauseated and/or diaphoretic and may demonstrate a horizontal nystagmus. The nystagmus will typically beat away from the involved side. Although, irritative lesions have been described early in the course of the disease with the nystagmus beating back toward the affected side.21
The progressive vestibular injury will also lead to a diminished vestibulo-ocular reflex on head thrust testing as well as rotation to the affected side on Fukuda testing. The endolymphatic hydrops may also result in a positive fistula test with pneumatic otoscopy as well as a Tulio phenomenon.
Diagnostic Criteria
With such varied presentation with fluctuating symptoms, the diagnosis of Meniere disease can often be difficult to make. In response to these challenges, the Academy of Otolaryngology-Head and Neck Surgery Committee on Hearing and Equilibrium has published guidelines for the diagnosis of Meniere disease, most recently published in 1995 (Table 23.1). This was done, in large part, to allow for more standardization in reporting of Meniere’s research.
Definition of Vertigo in Meniere Disease
The 1995 guidelines gave specific definition regarding the character of vertigo seen in Meniere disease, termed episodic vertigo of the Meniere type. This is defined as:
Table 23.1 AAO-HNS CHE Guidelines: Diagnosis of Meniere Disease
Certain Meniere disease • Definite Meniere disease plus histopathologic confirmation Definite Meniere disease • Two or more definitive spontaneous episodes of vertigo lasting 20 min or longer • Audiometrically documented hearing loss on at least one occasion • Tinnitus or aural fullness in the treated ear • Other causes excluded Probable Meniere disease • One definitive episode of vertigo • Audiometrically documented hearing loss on at least one occasion • Tinnitus or aural fullness in the treated ear • Other causes excluded Possible Meniere disease • Episodic vertigo of the Meniere type without documented hearing loss, or • Sensorineural hearing loss, fluctuating or fixed, with disequilibrium but without definitive episodes • Other causes excluded |
Adapted from reference 22.
AAO-HNS CHE, American Academy of Otolaryngology-Head and Neck Surgery Committee on Hearing and Equilibrium; min, minutes.
Spontaneous rotational vertigo lasting at least 20 minutes (commonly several hours), is often prostrating, and is accompanied by disequilibrium, which may last for days. It is usually accompanied by nausea and commonly by vomiting or retching. Consciousness is not lost. During the definitive episode, horizontal or horizontal rotatory nystagmus is always present.22
Hearing Loss in Meniere Disease
According to the CHE guidelines, sensorineural hearing loss must be documented in the affected ear on at least one occasion according to at least one of the following scenarios:
• The average hearing thresholds at 0.25, 0.5, and 1 kHz is 15 dB or more, higher than the average of 1, 2, and 3 kHz.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


