Medial Maxillectomy, Open
Ehab Hanna
INTRODUCTION
Medial maxillectomy involves removal of the lateral nasal wall and the adjoining maxillary bone medial to the plane of the infraorbital nerve. A complete sphenoethmoidectomy is also usually performed. This can be accomplished using a transfacial exposure (lateral rhinotomy), sublabial approach (facial degloving), or endoscopic endonasal approaches. This chapter discusses in detail the transfacial exposure using the lateral rhinotomy incision, which is the most widely practiced surgical approach for medial maxillectomy.
HISTORY
Small intranasal tumors are often completely asymptomatic or mimic more common benign conditions such as chronic sinusitis, allergy, or nasal polyposis. Since early detection of sinonasal tumors is probably the most important factor in improving prognosis, a high degree of suspicion is necessary to diagnose smaller lesions. Common symptoms include nasal obstruction, “sinus pressure” or pain, nasal discharge that may be bloody, anosmia, or epistaxis. Failure of these symptoms to respond to adequate medical therapy or, particularly, the presence of unilateral signs and symptoms should alert the physician to the possibility of a neoplasm and warrants further investigation by high-resolution imaging.
Extension of sinonasal tumors to adjacent structures renders the diagnosis obvious but is a late manifestation of the disease. Epiphora usually indicates obstruction of the nasolacrimal duct by tumor compression or direct invasion. Diplopia may be due to upward or lateral displacement of the globe by the tumor or more ominously due to invasion of the extraocular muscles. Blurred or reduced vision may indicate involvement of the optic nerve. Numbness or tingling of the cheek may be a symptom of perineural spread along the infraorbital nerve.
PHYSICAL EXAMINATION
Comprehensive examination of the nasal cavity should be done after topical decongestion and anesthesia using rigid or flexible endoscopy (Fig. 17.1). The presence of intranasal masses, ulcers, or areas of contact bleeding should be noted. Although unilateral “polyps” may be inflammatory, they are more commonly neoplastic. Tumors may also present as a submucosal mass without changes in the mucosa, other than displacement. Any suspicious lesions should be biopsied, preferably after high-resolution imaging has been obtained to avoid severe bleeding and/or cerebrospinal fluid (CSF) leak.
Detailed examination of the head and neck may reveal signs of extension of the tumor to adjacent structures. Soft tissue swelling of the face may indicate tumor extension through the anterior bony confines of the nose and sinuses. Inferior extension toward the oral cavity may present with an ulcer or a submucosal mass
in the palate or the alveolar ridge. Middle ear effusion may indicate tumor involvement of the nasopharynx, Eustachian tube, pterygoid plates, or tensor veli palatini muscle. Extension to the skull base may lead to involvement of the cranial nerves resulting in anosmia, blurred vision, diplopia, or hypoesthesia along the branches of the trigeminal nerves. The presence of an associated mass in the neck may represent cancer metastatic to the cervical lymph nodes.
in the palate or the alveolar ridge. Middle ear effusion may indicate tumor involvement of the nasopharynx, Eustachian tube, pterygoid plates, or tensor veli palatini muscle. Extension to the skull base may lead to involvement of the cranial nerves resulting in anosmia, blurred vision, diplopia, or hypoesthesia along the branches of the trigeminal nerves. The presence of an associated mass in the neck may represent cancer metastatic to the cervical lymph nodes.
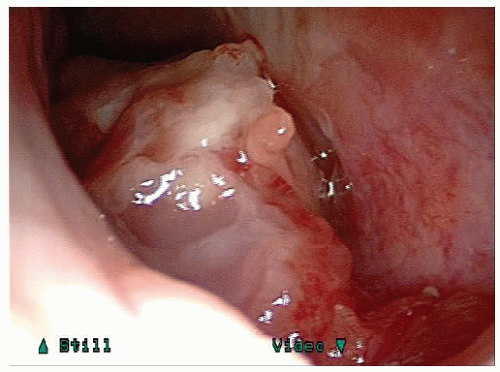 FIGURE 17.1 Endoscopic view of a tumor arising from the floor of the right nasal cavity. Biopsy revealed squamous cell carcinoma. |
Evaluation of the patient with a sinonasal neoplasm and suspected extension into the orbit should include a detailed neuro-ophthalmologic examination. This usually includes detailed assessment of visual acuity, visual fields, and ocular motility.
INDICATIONS
The most common indication for medial maxillectomy is in the treatment of tumors involving the nasal cavity, lateral nasal wall, ethmoid/sphenoid sinuses, and medial maxillary sinus (Fig. 17.2). The mucosal lining of the nose includes the respiratory epithelium composed of pseudostratified ciliated columnar epithelium with goblet cells, which may give rise to squamous cell carcinoma and adenocarcinomas. These are the most common sinonasal cancers in the United States and Europe, respectively.
The olfactory epithelium gives rise to olfactory or esthesioneuroblastoma. Other neuroendocrine tumors include neuroendocrine carcinomas, sinonasal undifferentiated carcinoma (SNUC), schwannomas, and peripheral
neuroectodermal tumors. The Schneiderian epithelium gives rise to Schneiderian (inverted) papillomas and carcinoma. Minor salivary gland tumors include adenoid cystic and mucoepidermoid carcinomas. Melanocytes within the nasal mucosa can give rise to sinonasal melanoma. Nonepithelial tumors arising from the sinonasal region include juvenile nasopharyngeal angiofibroma, hemangiopericytoma, sarcomas, and fibro-osseous lesions such as fibrous dysplasia, ossifying fibromas, and giant cell tumors. The differential diagnosis of sinonasal neoplasms is detailed in Table 17.1.
neuroectodermal tumors. The Schneiderian epithelium gives rise to Schneiderian (inverted) papillomas and carcinoma. Minor salivary gland tumors include adenoid cystic and mucoepidermoid carcinomas. Melanocytes within the nasal mucosa can give rise to sinonasal melanoma. Nonepithelial tumors arising from the sinonasal region include juvenile nasopharyngeal angiofibroma, hemangiopericytoma, sarcomas, and fibro-osseous lesions such as fibrous dysplasia, ossifying fibromas, and giant cell tumors. The differential diagnosis of sinonasal neoplasms is detailed in Table 17.1.
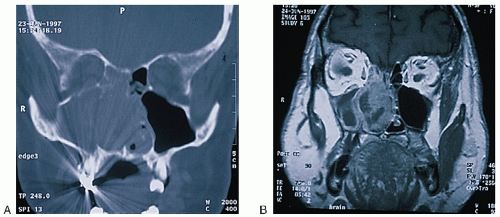 FIGURE 17.2 A: Coronal CT scan demonstrating opacification of the right nasal cavity as well as the maxillary and ethmoid sinuses. There appears to be destruction of the lateral nasal wall and the nasal septum. The lesion is abutting the orbital floor and the cribriform plate, but it is unclear whether or not these structures are involved. B: Coronal T1-weighted MRI with gadolinium of the same patient revealing that the lesion is limited to the nasal cavity and ethmoid sinuses and that the changes in the maxillary sinuses are due to retained secretions secondary to obstruction of the ostium, rather than soft tissue involvement. It also demonstrates that the lesion does not invade the orbit or the cranial base. |
TABLE 17.1 Tumors of the Sinonasal Tract | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||



