Medial Maxillectomy, Endoscopic
Carl H. Snyderman
INTRODUCTION
The medial maxilla separates the maxillary sinus from the nasal cavity, and medial maxillectomy has traditionally been performed to approach tumors both benign and malignant that involve the lateral nasal wall. Access is typically provided by a lateral rhinotomy or midfacial degloving approach. Excellent results have been achieved in the treatment of inverting papillomas with such an approach. Limitations of the lateral rhinotomy, however, are visualization of intranasal anatomy and the morbidity of a facial incision.
The advent of nasal endoscopy for the treatment of inflammatory sinonasal disease has resulted in the application of endoscopic techniques to the management of sinonasal neoplasms. Abundant clinical experience has confirmed that benign tumors such as inverting papillomas can be resected endoscopically with comparable outcomes and less morbidity. Endoscopic medial maxillectomy can also be applied to other benign tumors such as angiofibromas and selected sinonasal malignancies.
HISTORY
The symptoms of a sinonasal tumor are often nonspecific and include nasal obstruction, epistaxis, epiphora, hearing loss, and sinus headache. Patients often have symptoms for weeks to months and undergo multiple courses of medical treatment for allergies or sinusitis before an accurate diagnosis is made. Symptoms that suggest tumor extension beyond the nasal cavity include facial hypesthesia, visual symptoms, trismus, loose teeth, and facial swelling. Patients should be queried about visual acuity, diplopia, and sensation of the face and palate.
PHYSICAL EXAMINATION
The physical examination should include a complete examination of the head and neck supplemented with nasal endoscopy. Inspection of external features looks for asymmetry and inflammatory changes. Examination of the eyes includes an assessment of visual acuity, extraocular motility, and proptosis. Swelling inferomedial to the medial canthus may be secondary to dacryocystitis from tumor obstruction of the nasolacrimal duct or tumor growth along the duct. Otoscopy may demonstrate retraction of the tympanic membrane or a middle ear effusion. A large tumor in the nasal cavity may be evident without endoscopy, but endoscopy adds additional information regarding the origin of the tumor and areas of invasion. Nasal endoscopy establishes the vascularity of the tumor and coexistent pathology such as nasal polyposis or sinusitis. Examination of the oral cavity may reveal edema of the mucosal tissues of the hard palate on the side of the tumor. A large tumor may displace the soft palate and result in thick nasopharyngeal drainage. Palpation of the maxilla and intraoral mucosa is important to assess extension beyond the nasal cavity into the soft tissues. The neck is examined for evidence of cervical metastases. This is rare with sinonasal malignancy, and it may be difficult to distinguish between inflammatory and neoplastic lymphadenopathy. Assessment of cranial nerve function includes olfaction, eye
function (visual acuity and ocular motility), and trigeminal nerve function [sensory (V2, V3) and motor (V3)]. Olfaction can be assessed using subjective or objective (UPSIT Sensonics test) measures.
function (visual acuity and ocular motility), and trigeminal nerve function [sensory (V2, V3) and motor (V3)]. Olfaction can be assessed using subjective or objective (UPSIT Sensonics test) measures.
INDICATIONS
Medial maxillectomy is performed for the removal of benign and malignant tumors that involve the lateral nasal wall/medial maxilla and to gain access to tumors in the masticator space and infratemporal skull base (floor of middle cranial fossa). The amount of lateral exposure is dependent on the extent of the medial maxillectomy. Addition of an anteromedial maxillectomy (Denker approach) provides maximal access; lateral limits are the mandibular ramus and temporomandibular joint.
Tumors typically requiring a medial maxillectomy include sinonasal malignancies, such as squamous cell carcinoma, adenocarcinoma, adenoid cystic carcinoma, melanoma, and undifferentiated carcinoma. Inverting papillomas require a medial maxillectomy due to their origin from the lateral nasal wall. The most common tumor that requires a medial maxillectomy for surgical access is the angiofibroma. These tumors typically extend between the medial and lateral pterygoid muscles. Other tumors in the masticator space include benign tumors of neurogenic origin such as neurilemmomas and neurofibromas.
CONTRAINDICATIONS
The floor of the maxillary sinus is at a lower level than the nasal floor, and a medial maxillectomy approach will provide limited access to this region if there is tumor involvement. Similarly, tumor extension to the anterior wall of the maxilla is better handled with an anterior transmaxillary approach. Large invasive cancers with involvement of superficial tissues are better managed with an open approach. Depending on the reconstructive needs, an open approach may also be more expedient. For example, if a temporalis muscle transposition is indicated for protection of the skull base or internal carotid artery, an infratemporal skull base approach will provide access for resection as well as reconstruction. Finally, for large tumors, such as angiofibroma, an open approach may provide more room for instrumentation (bayonet bipolar electrocautery, powered instrumentation of the tumor).
PREOPERATIVE PLANNING
Computed tomographic (CT) scans provide the most information regarding sinus anatomy and the interface between air and soft tissue/bone. Destruction of bone can occur from slow remodeling from benign processes or infiltration from malignancy. Magnetic resonance imaging (MRI) is superior for soft tissue margins when tumor extends beyond bone boundaries (orbit, masticator space) and for detection of perineural invasion. T2-weighted sequences can help differentiate mucus secretions from tumor in obstructed sinuses. Contrast enhancement of CT and MRI scans is used to distinguish benign and malignant tumors from normal tissues and establish a differential diagnosis.
If the tumor is highly vascular or extends lateral to the maxilla, preoperative angiography with embolization of the internal maxillary artery (IMA) is considered. For vascular tumors, our preferred material for embolization is Onyx (Micro Therapeutics, Inc., Irvine, CA). The proximal IMA is also occluded with coils. Even when the tumor is not hypervascular, preoperative occlusion of the IMA facilitates dissection in the masticator space without concern for vascular injury.
SURGICAL TECHNIQUE
Endoscopic medial maxillectomy varies in the amount of exposure and extent of access provided. The exposure is tailored to the needs of the operation. The patient is positioned in a supine position. If intraoperative navigation is planned, registration of the navigation system is performed at this time. If immobilization of the head is desired or it is difficult to maintain the head in the desired position, the head is placed in three-point fixation with a Mayfield head holder. Topical vasoconstriction of nasal mucosa is achieved with intranasal pledgets soaked in 0.05% oxymetazoline. Standard antibiotic prophylaxis consists of intravenous administration of a second-generation cephalosporin. The nasal vestibule and surrounding skin are prepped with a Betadine solution; antiseptic prepping of the nasal cavity or oral cavity is not necessary.
Endoscopic Middle Meatal Antrostomy (Fig. 18.1A)
The middle turbinate is medialized or partially resected if there is a large concha bullosa. The uncinate process is palpated and the site of attachment to the inferior turbinate is visualized. The uncinate process is resected with backbiting forceps, and the opening is maximally enlarged anteriorly until dense bone is encountered,
inferiorly to the attachment of the inferior turbinate, and posteriorly to the sphenopalatine foramen (Fig. 18.2). Care is taken to avoid injury to the nasolacrimal duct anteriorly.
inferiorly to the attachment of the inferior turbinate, and posteriorly to the sphenopalatine foramen (Fig. 18.2). Care is taken to avoid injury to the nasolacrimal duct anteriorly.
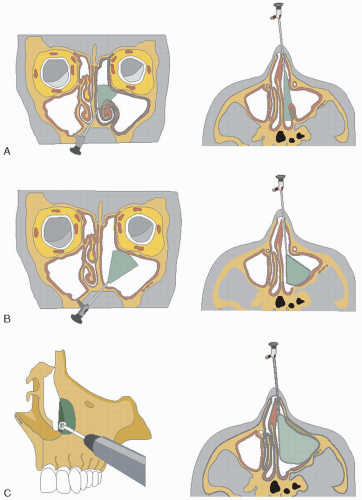 FIGURE 18.1 Extent of maxillary opening and visualization provided by (A) middle meatal antrostomy, (B) medial maxillectomy, and (C) medial maxillectomy and anteromedial maxillotomy. |
An endoscopic middle meatal antrostomy provides access to the medial aspect of the pterygopalatine space. The mucoperiosteum of the lateral nasal wall is elevated from the bone at the posterior margin of the antrostomy. The sphenopalatine artery exits the sphenopalatine foramen at the posterior-superior corner of the maxillary sinus. A useful landmark is the crista ethmoidalis, a small crest of bone just superficial to the foramen. The foramen is enlarged with a 1-mm 45-degree Kerrison rongeur to avoid injury to the vessel. Removal of bone continues laterally to expose the contents of the pterygopalatine space. This exposure is a prerequisite for an endoscopic transpterygoid approach.
A Silastic nasal splint is sutured to the nasal septum to prevent postoperative synechiae. Additional packing is only necessary if there is continued bleeding.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


