(1)
Alo Eye Care, Kolkata, India
Keywords
Canthal reconstructionFull-thickness skin graftsAdvancement flaps‘V’ to ‘Y’ Glabellar rotation flapMidline forehead flapCheek rotation flap14.1 General Considerations
Management of tumors involving the medial canthus are a bit challenging.
There usually is no lid margin tissue present, so determining how deep the tumor has spread is difficult.
Another issue is the presence of the lacrimal drainage system as part of, as well as close to, the medial canthus.
As a principle, microscopically tumor-free margins are required; therefore, management must be aggressive, even if part or all of the lacrimal drainage channels have to be sacrificed.
Repair of a medial canthus tissue defect may range from simple small patch skin and subcutaneous tissue loss to complex medial canthal reconstruction, along with repair of the lacrimal drainage channels.
14.2 Basic Principles
If the medial canthal ligament has been disrupted during surgical excision, telecanthus tends to form during healing. An attempt should be made to appose the medial canthal ligament or, if the medial end is not clearly delineated, to at least transfix the lateral end of the ligament to the soft tissue at the area of medial canthal insertion over the medial orbital margin.
When any skin defect is replaced with a flap or graft in the region of the medial canthus, deeper transfixion sutures should be applied to the region of the deeper medial canthal tendon. This approach provides a better, natural concavity to the medial canthal area. In addition, it reduces any free space between the graft and the underlying tissue, resulting in better acceptance.
If the whole lacrimal sac must be sacrificed to make the area tumor-free, the lacrimal drainage channels should not be reconstructed as a primary procedure. If epiphora occurs, reconstruction may be performed postoperatively.
If only a part of the lower canaliculus is excised, the monocanalicular or bicanalicular lacrimal tube may be kept in place.
If the cut end of the lower canaliculus can be located clearly, it may be sniped and marsupialized with the surrounding conjunctival sac, which works quite well.
If the upper canaliculus must be removed, it need not be reconstructed.
The spontaneous granulation, or laissez-faire, technique, which basically is healing by secondary intent with granulation tissue, is useful if the canthal margin is not involved. Little healthy tissue is available for flap mobilization, especially in cases involving visible bare periosteum, which have a very high graft rejection rate.
14.3 Full-Thickness Skin Grafts
14.3.1 Indications
Full-thickness skin grafts will provide good results for medial canthal area defects, preferably those not involving the canthal margin and those with a good underlying vascular bed.
14.3.2 Technique
A full-thickness skin graft is taken based on the template of the tissue defect.
The graft is placed over the defect. For better fixation, a deep suture is placed between the deeper tissue of the skin graft and the underlying bed. It is fixed at the margin with 6/0 nonabsorbable interrupted sutures.
A bolster is applied over the graft and kept in position for 5–7 days.
The marginal sutures are removed after 7–10 days.
14.3.3 Other Variations/Options
An advancement or rotational flap is an alternative, especially in situations in which the underlying bed is not very vascular.
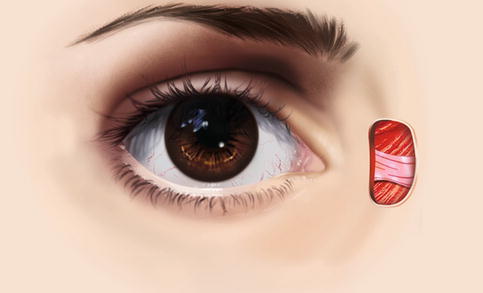
Fig. 14.1
Full-thickness skin graft. An anterior lamellar defect of the skin over the medial canthus
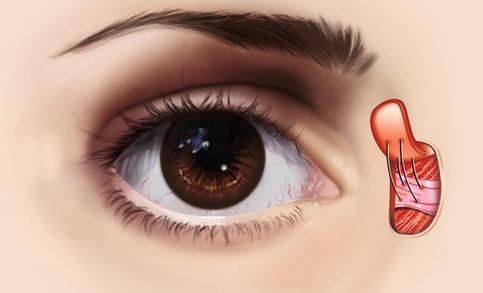
Fig. 14.2
Full-thickness skin graft. A full-thickness skin graft is taken based on the template of the tissue defect and is placed over the defect. A deep suture is placed between the deeper tissue of the skin graft and the underlying bed, for better fixation
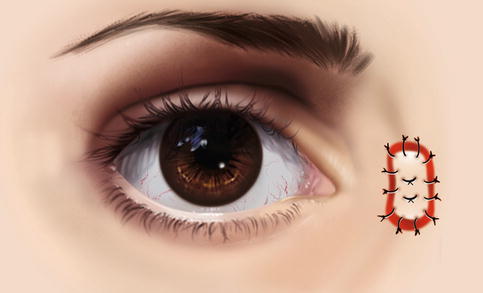
Fig. 14.3
Full-thickness skin graft. The graft is fixed at the margin with 6/0 nonabsorbable interrupted sutures
14.4 Advancement Flaps
14.4.1 Indications
Cases in which enough healthy and loose skin is available in the superior medial and inferomedial periorbital regions.
Tissue defects that are not very large.
14.4.2 Technique
Two parallel skin markings are made circumferentially above and below the tissue defect. The marks follow the contour of the underlying orbicularis muscle in the periorbital region.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


