(1)
St. Johns, FL, USA
(2)
Helen Keller Foundation for Research and Education, International Society of Ocular Trauma, Birmingham, AL, USA
(3)
Consultant and Vitreoretinal Surgeon, Milos Eye Hospital, Belgrade, Serbia
(4)
Consultant and Vitreoretinal Surgeon, Zagórskiego Eye Hospital, Cracow, Poland
14.1 Air1
Air is a great intraoperative tool for several reasons:
It forces to the deepest point of the eye the intravitreal/subretinal fluid, allowing its drainage.
It provides instant tamponade for a retinal break.2
It keeps the retina attached, even if the IPM has been broken.
It acts as a lens, providing the surgeon a wider field of view than under fluid.
In the AC, it has the following benefits:
Instant deepening of the AC.
Prevention of the formation of anterior synechia.
Highlighting the presence of prolapsed vitreous4
Air helps demonstrate the presence of vitreous behind the posterior capsule (see Sect. 27.5.3).
Complications 5: When A-F X is performed in the presence of RD, there is a danger of small air bubbles (“fish eggs”) getting under the retina or the air tearing a retina that is under severe traction or is shortened (similar to that seen with gas use, see Sect. 54.4.2.9).
The risk of high IOP or cataract is less pronounced with air than with gas (see below) because it is nonexpansile and gets absorbed in a few days.
Pearl
A rarely mentioned side effect of the use of intravitreal air and gas is that most patients cannot see through them. If they are not told about this in advance, it may be a very scary experience – another example of the importance of proper counseling (see Chap. 5).
14.2 Intravitreal Gas
Gases are used to provide tamponade that lasts several days to a few weeks.
Depending on their concentration, gases can be nonexpansile or expansile. They are assumed to work via their tamponading effect (“covering the retinal break”) in eyes with an RD (see the remark above) or macular hole.
SF6: It doubles its volume if pure gas is used. The typical concentration is ~30%, which lasts for up to 2 weeks.
C3F8: It increases its volume 4 times if pure gas is used. The typical concentration is ~15%, which lasts for up to 2 months.6
With the patient being at reduced atmospheric pressure,7 even a gas with a nonexpansile concentration expands, and this effect is proportional to the outside pressure; IOP elevation results.
Such an IOP elevation would also occur during general anesthesia as the N2O used enters the vitreous cavity. The vitrectomy machine prevents this pressure rise by automatically adjusting the IOP, but if the anesthetic gas is not allowed to escape8 from the vitreous before surgery is completed, the gas tamponade will be short-lasting because that gas escape occurs postoperatively.
Gases can also be used in the AC in eyes with severe hypotony. They increase the IOP for a few days if a nonexpansile, or even weeks if expansile, concentration is used.
Complications 9: High IOP (see above) and cataract; the latter (“gas cataract”) may be temporary (see Fig. 14.2). Rarely, a visual field defect develops.10 Gases may also enter the subretinal space, but this is less common than with air, due to the high surface tension of the gas.

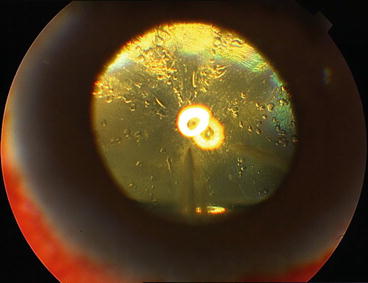
Fig. 14.1
Pneumovitrectomy for the “vitreous skirt” in the periphery. The image is slightly different in the air-filled eye if vitreous is still present. On the left side, pneumovitrectomy has already been done and the remaining vitreous skirt is greatly trimmed; to the right, where the probe is held, the skirt is still rather thick. All this is readily visible under air; if BSS is used, the remaining vitreous is largely unnoticeable
Fig. 14.2
Gas cataract. Typical image of the lens feathering due to long vitrectomy or gas implantation. With very rare exceptions, the condition resolves spontaneously with time
14.3 Silicone Oil
Providing long-term11 tamponade, the oil can be both a prophylactic and a therapeutic tool.
Table 14.1
Duration options of silicone oil tamponade
Duration | Common conditionsa | Comment |
|---|---|---|
Weeks | Macular hole | This period should be sufficiently long to achieve hole closureb; if the hole remains open after a month or so, it is unlikely to close even if the silicone oil is retained for longer |
Monthsc | RD | Large (giant) or multiple breaks, unsuccessful RD surgery on the fellow eye Typical duration of tamponade: at least 3 months |
PVR present | The most effective weapon to keep the retina attached. Having significant amount of pigment in the vitreous is an indicator of more severe PVR to develop (see Fig. 53.1) Typical duration of tamponade: 3–6 months | |
PVR expected (prophylaxis) | The silicone oil acts as a space-occupying tool Typical duration of tamponade: ~3 months | |
PDR | The most effective weapon to keep the retina attached; the oil also helps prevent VH Typical duration of tamponade: 3–6 months | |
Endophthalmitis | If the retina is detached or damaged (break/s, necrosis) or if, due to the reaccumulation of debris, postoperative visibility of the retina is expected to be poor Typical duration of tamponade: ~3 months | |
Permanent (forever)d | Recurrent/nontreatable RD | The oil is the only tool that may be able to prevent further deterioration of the condition (RD, recurrent VH). Periodically, the silicone oil must be exchanged |
Severe hypotony, phthisical eye | The oil is the only tool that may be able to prevent further deterioration of the condition. Periodically, the silicone oil must be exchanged It is best to make the eye aphakic and the “100% fill” means 100% for the entire eyeball, not only the vitreous cavitye |
14.3.1 Types of Silicone Oil
Viscosity: The two typical options are 1,000/1,300 cst and ≥5,000 cst.
Higher viscosity is assumed to delay the time to emulsification.12
The higher the viscosity, the more difficult to inject, and especially extract, the oil.
Molecular weight: Standard vs “heavy” silicone oil.
The standard oil13 has a specific gravity of 0.97: it floats on water (BSS, aqueous).
The “heavy” oil has a specific gravity of 1.02–1.06: it sinks in water (BSS, aqueous).
14.3.2 Achieving a 100% Fill14
The oil is supposed to be in contact with the retina,15 ciliary body, zonules, and the posterior capsule (iris in the aphakic eye) over their entire surface. To achieve this, the surgeon needs to do the following.
Q&A
Q
What is the true benefit of a 100% silicone oil fill?
A
In principle, cells cannot accumulate and proliferative membranes cannot form: the risk of PVR development is reduced.
Fig. 14.3
The double-loop suture to close the sclerotomy to avoid silicone oil loss. (a) Entry (1, 3) and exit (2, 4) points of the needle; the numbers represent the proper sequence. (b) The appearance of the suture once the threads have been cut
If the fill is incomplete, a crescent of aqueous is found, in the erect patient, at the bottom of the eye.19 Inflammatory debris collects in this pool of fluid, increasing the risk of PVR.
Pearl
The use of heavy silicone oil shifts the pool of fluid superiorly. With the use of standard oil, the PVR starts inferiorly; it is shifted superiorly with heavy oil (see Table 14.2).
Table 14.2
Clinical implications of an underfill with silicone oils of different weight
Variable | Standard oil | Heavy oil |
|---|---|---|
Consequence: always | Fluid pooling inferiorly | Fluid pooling superiorly |
Consequence: potentially | Cell proliferation, membrane formation inferiorly PVR/RD inferiorly with a relative visual field defect superiorly | Cell proliferation, membrane formation superiorly PVR/RD superiorly with a relative visual field defect inferiorly |
Reoperation for PVR/RDa | Retinectomy (+silicone oil reimplantation) | Retinectomy (+silicone oil reimplantation) |
Reoperation: Implications for patient | Partial loss of the upper visual field (less important in everyday life, but the loss may be rather extensive due to multiple retinectomies) | Partial loss of the lower visual field (more important in everyday life, but the loss may be less extensive if the previous retinectomy was inferior) |
Reoperation: Implications for surgeon | Technically, access to all of the inferior retina is rather easy | Technically, access to the superior retina is more difficult |
Removal of the oil | Technically easy | Technically more difficult |
With silicone oil use, there are important questions related to the lens20 (see Table 14.3).
Table 14.3
Silicone oil and the lens
Issue/question
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|
|---|