and Charles P. Molumi2
(1)
University of Papua New Guinea and Port Moresby General Hospital, Boroko, National Capital District, Papua New Guinea
(2)
Port Moresby General Hospital, Boroko, National Capital District, Papua New Guinea
7.1 Mandibulotomy for Access

Fig. 7.1
The incision for midline mandibulotomy is marked out running in the midline of lower lip to the level of the hyoid and laterally to the anterior border of sternocleidomastoid muscle and up to the mastoid process. In the oral cavity the incision is made along the medial border of the mandible in the midline to the retromolar trigon area

Fig. 7.2
Mandibulotomy is done in the midline. The soft tissue attachments to the floor of mouth to the mandible are excised and the mandible is reflected laterally pivoting at the temporomandibular joint
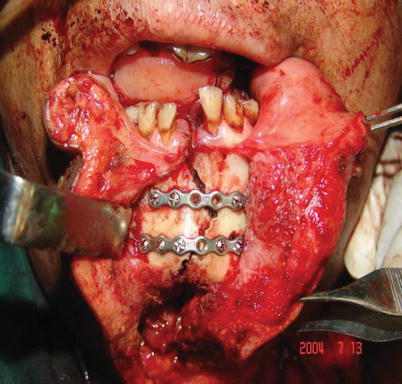
Fig. 7.3
After the procedure, the temporomandibular joint is checked for dislocation and the mandible placed back in position and held together with mini plate and screws
7.2 Segmental Mandibulectomy and Reconstruction with Stabilizing Plate and Screw
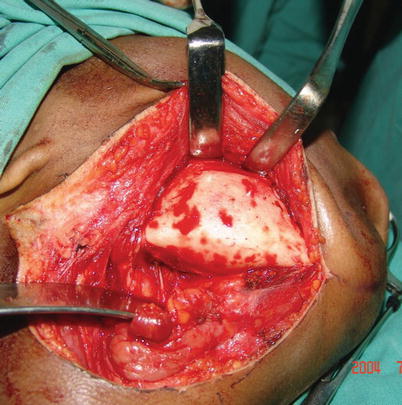
Fig. 7.4
Through an incision two finger breaths below the angle of mandible, the mandibular tumor is exposed and marked out for segmental mandibulectomy
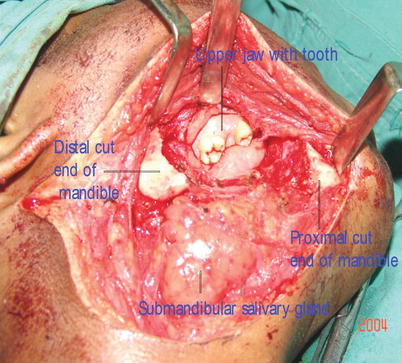
Fig. 7.5
The proximal and distal ends of the mandible are exposed after mandibulectomy and freed of any tissue attachments in preparation for plating

Fig. 7.6
Stabilization plate are placed and held in place with screws placed at the proximal and distal cut ends of the mandible
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


