CHAPTER 47 Management of trichiasis/distichiasis
Definition of trichiasis
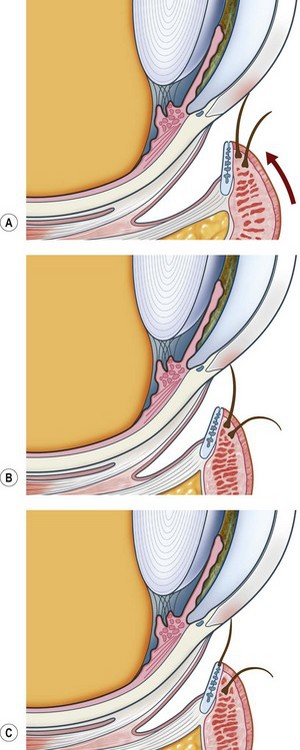
Trichiasis is defined as an eyelash that touches the eye but arises from the anterior aspect of the lid margin. It is distinguished from ‘aberrant’ lashes that arise from the meibomian gland openings near the posterior lid margin and ‘misdirected’ lashes that arise from the lid margin and are abnormally directed. Distichiasis is a condition where lashes arise from the orifices of the meibomian glands. However, common parlance often uses the word ‘trichiasis’ to mean any or all of the above. The terms ‘lash-induced trichiasis’ and ‘lid-induced trichiasis’ are also in usage (Fig. 47.1).
Physiology of normal eyelash formation
Hair is formed by the replication of cells within the hair follicles1. Follicles may produce either ‘lanugo’ (fetal hair), ‘vellus’ or ‘terminal’ hairs. Eyelashes, eyebrows, scalp hair and pubic hair are all terminal hairs while vellus hair cover the rest of the body and is associated with ‘goose-pimples’ due to erector pili units. Eyelash follicles are located anterior to the tarsal plate, deep to orbicularis oculi and adjacent to the inferior or superior marginal arterial arcades. The upper lid follicles are deeper (1.8 vs. 1.0 mm) and the bulbs are wider (188 vs. 132 microns). The upper lid has twice the number of follicles2.
Hair growth occurs in a cyclical manner with the follicles undergoing growth, atrophy, and then inactivity; anagen, catagen, and telogen1. The duration of each phase of the cycle depends on the type of hair and its location. Eyelashes have an optimum length and this is regulated by the hair cycle. They grow for 10 weeks followed by a resting period of 9 months3. During the resting phase the lashes may be lost. This mechanism regulates the length of the lashes by stopping growth after they have reached the ‘correct length’. In comparison, scalp hairs grow for 2–6 years and then rest for 3 months. Therefore, scalp hair grows longer.
Pathophysiology of abnormal eyelash formation
Aberrant lashes are usually ‘stunted and non-pigmented’ and arise from the meibomian glands. They may be congenital as in distichiasis. Acquired aberrant lashes occur after prolonged lid inflammation such as occurs in Stevens–Johnston syndrome or ocular cicatricial pemphigoid (OCP). Scheie and Albert4 state that acquired aberrant lashes are due to ‘meibomian glands [which] become modified and take on an atavistic hair-bearing function.’ Most human body hairs are associated with sebaceous glands and eyelashes are atypical in that they are not. In contrast, histology of congenital distichiasis shows that the meibomian glands are absent or rudimentary and this is presumably different from the acquired form. These congenital distichiasis follicles can be at very distant locations within the tarsal plate and this is important to any subsequent focal treatments for ablation5.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


