The management of regional lymph nodes in thyroid carcinoma is guided by preoperative evaluation, histologic subtype, and often a consideration of data for potential benefit and morbidity of a neck dissection. The goal of lymphadenectomy is complete surgical resection of grossly evident metastatic disease and the removal of regional lymph node groups at highest risk for microscopic disease. Surgery should achieve disease eradication but preserve voice, airway, swallowing, and parathyroid function. This article discusses recommendations for addressing cervical lymph nodes in thyroid carcinoma, discusses current literature regarding the common histologic subtype (papillary carcinoma), and details our operative approach.
Key points
- •
Surgery should be tailored to achieve the oncologic goals of disease eradication while preserving voice, airway, swallowing, and parathyroid function.
- •
Although controversial, prophylactic central compartment (level VI) neck dissection for papillary thyroid carcinoma should be considered in certain circumstances (tumors > 4 cm or those with extrathyroidal extension).
- •
When indicated, functional or modified radical neck dissection for differentiated thyroid cancer generally includes lymphadenectomy of levels IIa, III, IV, and Vb of the neck.
- •
Empiric oral supplementation with elemental calcium and vitamin D is generally warranted after paratracheal and mediastinal lymph node dissection.
Introduction
For regional control of differentiated thyroid cancer (DTC), the goal of lymphadenectomy is the complete surgical resection of all grossly evident metastatic disease and the selective removal of regional lymph node groups at highest risk for microscopic disease. Moreover, surgery should be tailored to achieve the oncologic goals of disease eradication while preserving voice, airway, swallowing, and parathyroid function. Therefore, management of the neck or cervical lymphadenectomy is the preferred treatment to obtain regional control in patients with cervical lymph node metastasis detected on initial staging. Likewise, an aggressive surgical approach is warranted for recurrent regional metastasis, because complete resection of disease correlates with improved disease-free survival. This article discusses the central compartment dissection, lateral neck dissection, and dissection of the metastatic retropharyngeal lymphatic node. Preoperative and postoperative care are discussed and a review of the literature is presented to consider new refinements in surgical technique, as well as current controversies and evolving treatment approaches.
Introduction
For regional control of differentiated thyroid cancer (DTC), the goal of lymphadenectomy is the complete surgical resection of all grossly evident metastatic disease and the selective removal of regional lymph node groups at highest risk for microscopic disease. Moreover, surgery should be tailored to achieve the oncologic goals of disease eradication while preserving voice, airway, swallowing, and parathyroid function. Therefore, management of the neck or cervical lymphadenectomy is the preferred treatment to obtain regional control in patients with cervical lymph node metastasis detected on initial staging. Likewise, an aggressive surgical approach is warranted for recurrent regional metastasis, because complete resection of disease correlates with improved disease-free survival. This article discusses the central compartment dissection, lateral neck dissection, and dissection of the metastatic retropharyngeal lymphatic node. Preoperative and postoperative care are discussed and a review of the literature is presented to consider new refinements in surgical technique, as well as current controversies and evolving treatment approaches.
Lymphadenectomy for thyroid cancer
Approach to the management of cervical lymph nodes in thyroid cancer is guided by many factors, including the preoperative detection of metastasis. Ultrasonography of the central and lateral neck is recommended by the American Thyroid Association (ATA) and current National Comprehensive Cancer Network guidelines during the preoperative evaluation of most thyroid malignancies. Papillary carcinoma, the most common histologic subtype of thyroid cancer, is often metastatic to regional lymph nodes on pathologic review, and ultrasonography can suggest lymph node involvement in approximately one-third of patients. Although ultrasonography is more sensitive than physical examination, a substantial number of patients have microscopic disease found on pathology following neck dissection for clinically negative necks, especially in the central compartment. However, ultrasonography may be sufficient for the detection of clinically relevant disease in papillary thyroid carcinomas, and ultrasonography may be especially useful in evaluation of lymph nodes in the lateral neck. Preoperative ultrasonography can significantly affect the extent of surgery planned for papillary carcinoma, as well as other types of thyroid malignancies. The preoperative detection of lymph node involvement by either clinical examination or imaging can significantly clarify the goal of neck management and make clear the distinction between a prophylactic and therapeutic neck dissection. In review of current guidelines and existing literature, a therapeutic dissection of clinically apparent node compartments is generally recommended in the surgical management of most thyroid cancers.
Central Lymph Node Compartment
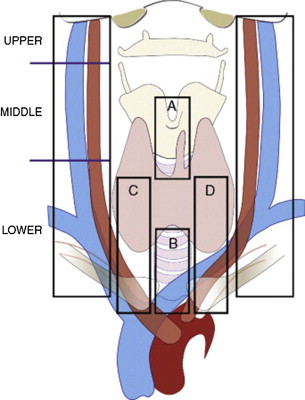
The central lymph node compartment (level VI) is frequently involved, and is bounded laterally by the carotid arteries, the hyoid bone superiorly, and the sternal notch (or the innominate artery if level VII is included) inferiorly ( Fig. 1 ). Lymph nodes within this compartment most commonly involved by metastatic thyroid carcinoma include the prelaryngeal (Delphian), pretracheal, and paratracheal nodes. An adequate unilateral central neck dissection, as defined by the ATA, should include the prelaryngeal, pretracheal, and the ipsilateral paratracheal nodal group. If performed with therapeutic intent, it is recommended that the dissection be extended to include bilateral paratracheal nodal groups. Other nodes within the central compartment that are less commonly involved include the retropharyngeal, retroesophageal, and paralaryngopharyngeal groups.
Lateral Node Involvement
Although metastatic thyroid carcinoma most frequently involves the central compartment, recent data have shown a high incidence of lateral nodal involvement, with pathologic metastasis in more than half of patients with papillary thyroid cancer and a similarly high number of patients with medullary carcinoma. Level III (ranging from the hyoid bone superiorly to the cricoid cartilage inferiorly and bounded by the sternohyoid medially and posterior border of the sternocleidomastoid laterally) is the most commonly involved lateral cervical group, but meta-analysis data have shown a high prevalence of multilevel disease, with levels II, III, IV, and V having metastatic involvement in 53%, 71%, 66%, and 25% of therapeutic neck dissections respectively for DTCs (see Fig. 1 ). The ATA has further reviewed the lateral neck dissection and recommends a therapeutic dissection of levels IIa, III, IV, and Vb when suspicious nodes are identified before surgery. The morbidity associated with further dissection of level V to include the superior portion of level Va (above the spinal accessory nerve) may be spared in the absence of clinically evident disease, because data show that this level is rarely involved.
Prophylactic Neck Dissection
Distinct from a therapeutic neck dissection, which most literature suggests is beneficial and generally recommended, is a prophylactic neck dissection, for which the indications are less clear. Existing data are heterogeneous in the demonstrated benefits and any associated morbidity of prophylactic central compartment neck dissection, especially in patients with papillary thyroid carcinoma.
In papillary carcinoma, current guidelines recommend considering a prophylactic central neck dissection if other factors in patient presentation prompt a total thyroidectomy. This position generally agrees with published recommendations from the ATA, which broadly suggest considering a prophylactic central neck dissection, especially in patients with advanced primary tumors larger than 4 cm. Again, papillary thyroid cancer is frequently metastatic to regional lymph nodes. In addition, the presence of lymph node metastasis may not be readily apparent on preoperative evaluation. However, the significance of this nodal involvement is less obvious. Several studies have shown that the pathologic identification of lymph node metastasis in papillary thyroid cancer can help predict disease-free and disease-specific survival and, thus, potentially help guide postoperative management. Although a prophylactic central lymph node dissection can offer information regarding prognosis, it is unclear whether it can be therapeutic. A review of literature documenting locoregional recurrence rates in clinically N0 patients with papillary thyroid carcinoma who underwent either total thyroidectomy (TT) alone or TT with concurrent prophylactic central neck dissections detailed a significant decrease (4.7% vs 8.6%) in recurrence rates when neck dissections were performed. However, this effect may be contributed to by an advancement of staging with pathologic information and an increased use of postoperative radioactive iodine (RAI). In addition, the benefit of a prophylactic central neck dissection in papillary thyroid cancer has not been uniformly documented, with some studies showing only a marginal decrease in recurrence rates. However, other work comparing patients with papillary carcinomas greater than 1 cm who uniformly received postoperative RAI following either TT alone or TT and a prophylactic neck dissection showed lower retreatment rates (either reoperation or additional RAI) in patients who underwent a neck dissection.
Any benefit, either prognostic or therapeutic, to a prophylactic central neck dissection may be partly tempered by associated morbidity. Although some series have shown that the inclusion of a prophylactic central compartment neck dissection only increases the risk of temporary hypocalcemia, other studies have documented an additional increase in temporary recurrent laryngeal nerve paralysis. These complications may be more closely associated with concurrent thyroidectomy than with the neck dissection. Regardless, the risks associated with the procedure, viewed in the context of uncertainty with regard to the improvement in outcomes, have led to the suggestion to consider a prophylactic central compartment neck dissection in papillary thyroid carcinomas that are either large tumors (>4 cm) or those with extrathyroidal extension.
Subtypes of Papillary Thyroid Carcinoma
There is much interest in further refining the approach to papillary thyroid carcinoma, which may eventually be dictated by molecular analysis of the primary tumor. At present, histologic analysis can offer some guidance in management. The different subtypes of papillary thyroid carcinoma are increasingly being recognized as distinct entities with differing biological behavior.
Follicular-variant papillary thyroid carcinoma (FV-PTC) is one of the most common variants of papillary carcinoma. It has the nuclear features of papillary carcinoma, but grows in a follicular architecture and has a high frequency of RAS point mutations, similar to other follicular carcinomas. Most FV-PTCs (excluding infiltrative subtypes) have a lower incidence of lymph node metastasis at presentation than classic papillary thyroid carcinomas. Recent literature suggests that a prophylactic central compartment neck dissection may be avoided in FV-PTCs. However, most FV-PTCs are diagnosed as such after surgery and other factors distinct from the histologic subtype often guide the decision to perform a prophylactic neck dissection. In select patients who undergo a thyroid lobectomy for papillary thyroid cancer, the diagnosis of FV-PTC may obviate further surgery, including a central neck dissection.
In contrast with papillary thyroid carcinoma, follicular thyroid cancer is less frequently metastatic to regional lymph nodes and, as such, a prophylactic central compartment neck dissection is rarely performed. Furthermore, because follicular carcinoma cannot be reliably diagnosed with fine-needle aspiration before surgery, the role of central neck dissection in this disease may be limited. For patients with tumors classified before surgery as follicular neoplasm and found to have cervical metastasis, the surgeon should consider the possibility of FV-PTC rather than the diagnosis of follicular carcinoma. Routine prophylactic central neck dissections for follicular carcinomas are therefore not recommended.
Hürthle cell carcinoma, an aggressive variant of follicular carcinoma, is often locally recurrent following primary resection with definitive intent. Similar to papillary thyroid carcinoma, current literature and recommendations support a therapeutic central and/or lateral compartment neck dissection for clinically involved nodes in Hürthle cell carcinoma and suggest considering a prophylactic central compartment neck dissection if a TT is prompted by other factors.
Medullary thyroid cancer is often metastatic to regional lymph nodes at presentation. In contrast with papillary thyroid cancer, in which the role of a prophylactic central neck dissection in the context of a clinically negative neck is less clear, routine central compartment neck dissection is recommended for patients with sporadic medullary thyroid cancer greater than 1 cm or patients with bilateral thyroid disease. Lateral neck dissection may be reserved for patients with clinically evident disease on preoperative examination or imaging. However, the presence of lateral cervical disease may not always be obvious before or even during surgery. In addition, there is a high rate of lateral cervical compartment microscopic disease in patients with involvement of the central compartment. Although patients with no pathologic involvement of the central neck have a low rate of lateral neck metastasis (10%), patients with even limited central involvement (1–3 positive nodes) have a high rate of lateral compartment disease. Thus, some clinicians have advocated for prophylactic lateral neck dissection when medullary carcinoma has spread to the central lymph node compartment.
Surgical technique
Central Compartment Dissection (Levels VI and VII)
Dissection of the central compartment includes lymphadenectomy of the pretracheal, paratracheal, and anterior mediastinal lymphoadipose tissues, all of which represent a potential first echelon of nodal drainage from the thyroid gland. Central compartment dissection is performed to remove clinically involved nodes or those at risk for metastatic disease based on features of the primary tumor.
For patients with papillary thyroid cancer, routine prophylactic central compartment dissection is not recommended. However, the thyroid surgeon should inspect and assess at-risk nodal echelons during TT and biopsy with frozen section any suspicious central compartment node to guide further surgical intervention. For patients with primary tumors greater than 4 cm, or with evidence of local invasion, an elective central compartment dissection may be indicated.
Surgical technique
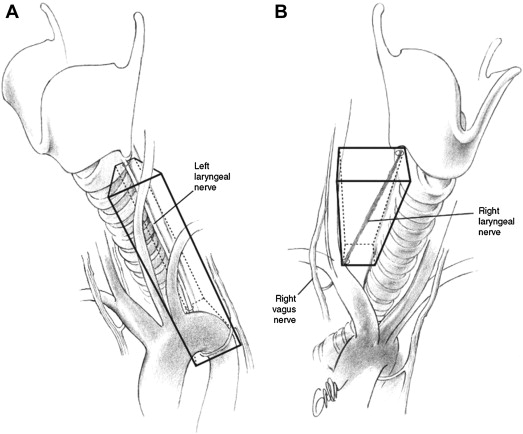
Central compartment dissection should encompass paratracheal, precricoid, and parathyroidal nodes located along the recurrent laryngeal nerves (level VI), as well as superior mediastinal nodes (level VII) ( Fig. 2 ). The craniocaudal extent of a central compartment dissection begins at the innominate artery below and ends at the hyoid bone above. The lateral extent of the central compartment dissection is the medial border of the carotid sheath. There are 3 critical but related objectives for this surgery.
- 1.
Once an indication for central compartment dissection has been confirmed, the surgeon should be as comprehensive as possible in removing nodes
- 2.
Preserve the anatomic integrity
- 3.
Minimize trauma to both the recurrent laryngeal nerves and vascularized parathyroid
- •
Central compartment dissection is performed after TT and begins by opening the carotid sheath from the hyoid bone to the proximal common carotid artery.
- •
In the right neck , the dissection is performed down to the origin of the right common carotid artery and its emergence from the brachiocephalic (or innominate) artery.
- •
The innominate artery is followed until the trachea is encountered.
- •
The right recurrent laryngeal nerve is identified as it emerges underneath the innominate artery then ascends superiorly from lateral to medial.
- •
In the left neck , because the left common carotid artery arises directly from the aortic arch, this great vessel provides a less reliable guide compared with the right. As a result, the common carotid artery is traced until the trachea is identified, usually at the level of the left brachiocephalic vein.
- •
The left recurrent laryngeal nerve takes a more medial course, ascending deep to the aortic arch and proximal common carotid artery.
- •
Upper mediastinal lymphoadipose tissue is then mobilized, because thyrothymic and the inferior thyroid veins must be individually clamped and ligated.
- •
This specimen is then swept superiorly to begin mobilizing the specimen.
- •
- •
With the ipsilateral nerve circumferentially dissected and with at least one vascularized parathyroid preserved, the remaining lymphadipose tissue is removed.
- •
Small-caliber vessels are managed with bipolar electrocautery, whereas larger vessels are suture ligated. The use of clips in this area is not recommended, because this practice confounds future computed tomography imaging of the paratracheal bed as well as future surgical intervention.