6 Management of Controlled Anterior Canal-Wall-Down Rehabilitation Middle Ear Obliteration Technique The different classifications of retraction pockets and cholesteatomas are directly related to the different dysfunctions of middle ear ventilation pathways (see Middle Ear Ventilation, p. 4).
Management of Retraction Pockets and Cholesteatoma
6__Management of Retraction Pockets and Cholesteatoma
Classification of Retraction Pockets (according to Gersdorff)
Noncholesteatomatous retraction pockets: | |
Type 1: | Mobile, reversible upon ventilation |
Type 2 a: | Adherent, self-cleaning, wholly visible with a microscope |
Type 2 b: | Wholly visible with an endoscope only |
Type 3: | Adherent, self-cleaning, beyond view with either the microscope or the endoscope (= precholesteatoma) |
Cholesteatomatous retraction pockets: | |
Type 4: | Adherent, not self-cleaning, with accumulation of keratin, epithelial debris (= cholesteatoma on retraction pocket) |
Type 5: | Adherent, not self-cleaning, with otorrhea and/or inflammatory granuloma (= infected cholesteatoma) |
Classification of Cholesteatomas
Mesotympanic
Protympanic
Retrotympanic
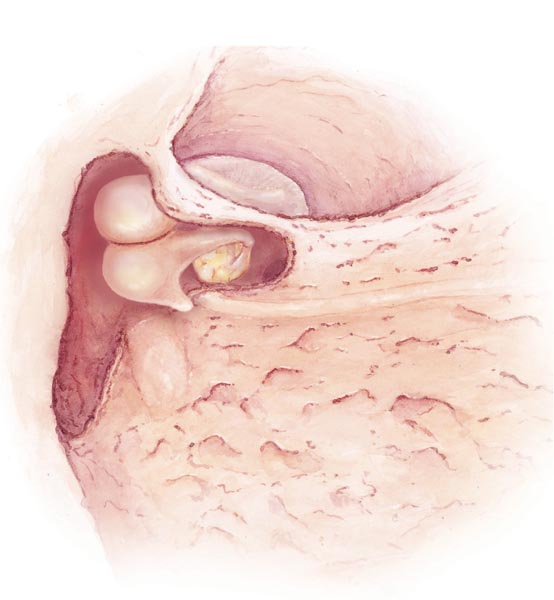
Fig. 6.1
Retrotympanic with Mastoid Extension
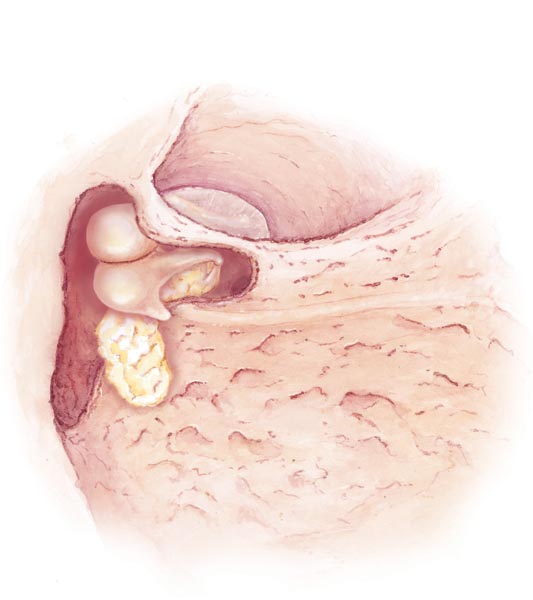
Fig. 6.2
Epitympanic
Anterior Epitympanic
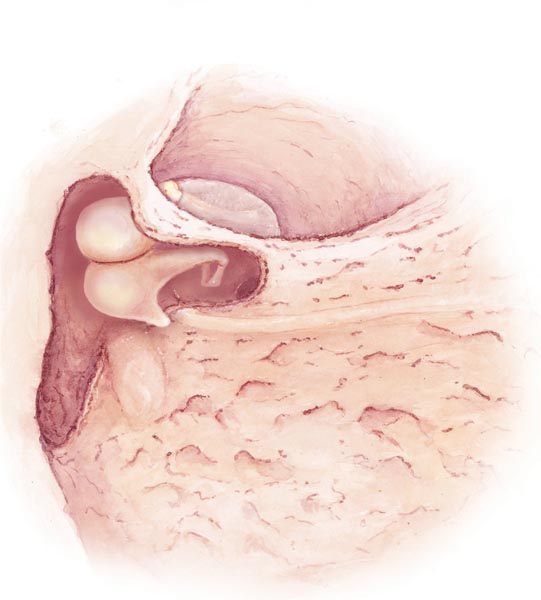
Fig. 6.3
Anterior Epitympanic with Medial Extension (Supratubal Fossa)
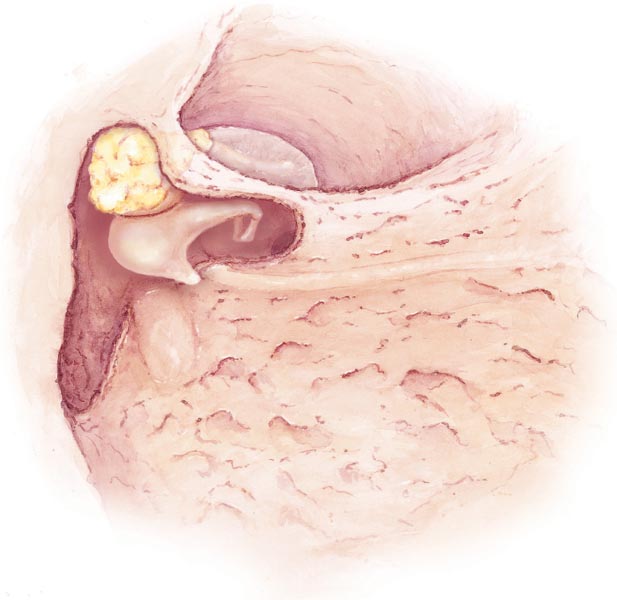
Fig. 6.4
Posterior Epitympanic
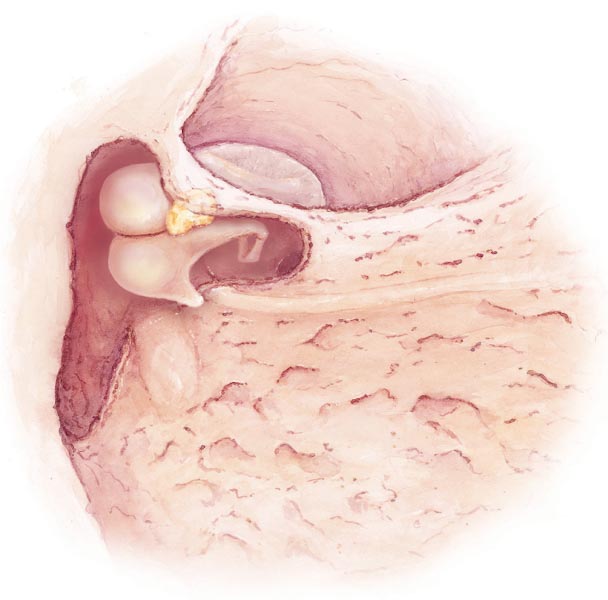
Fig. 6.5
Posterior Epitympanic with Mastoid Extension
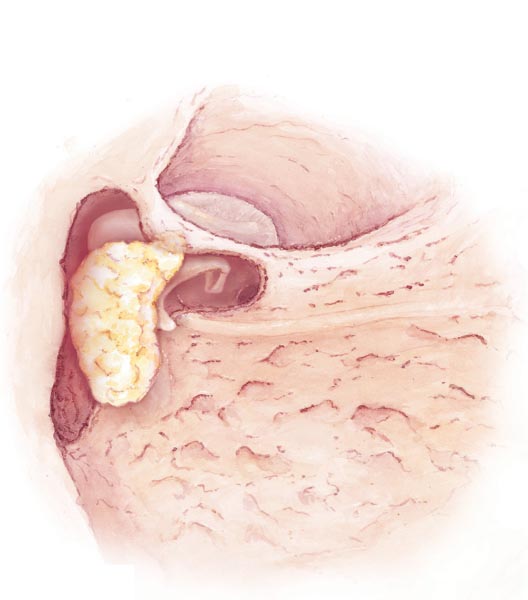
Fig. 6.6
Holotympanic
Holotympanic Starting from Retrotympanum or Posterior Attic with Mastoid Extension
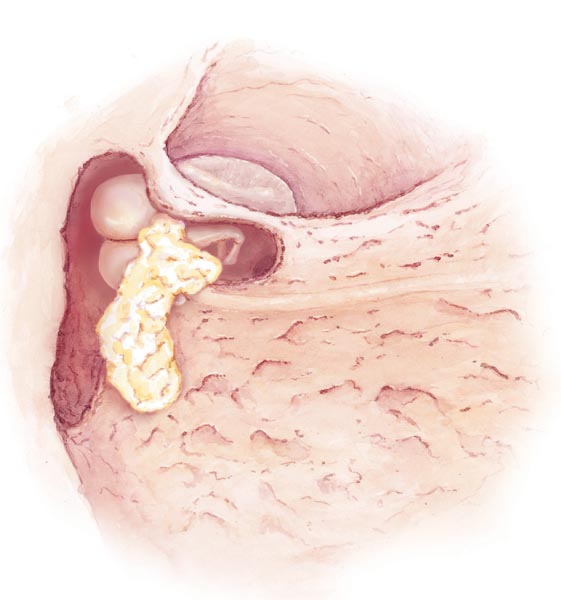
Fig. 6.7
Management Philosophy
Only retraction pockets with no self-cleaning properties and which show recurrent otorrhea and ossicular chain defects leading to significant conductive hearing loss should be operated on.
We perform mastoidectomy only for cholesteatomas of the mastoid cavity and for those originating in the tympanic cavity that cannot be satisfactorily managed by a transmeatal approach, with or without tympanoatticotomy.
In most cases, we use a canal-wall-up (CWU) technique, except in the case of very large defects of the external auditory bony canal wall eroding the mastoid, large recurrent or residual cholesteatomas, or large labyrinthine fistulas, or in patients with large cholesteatomas who are at high risk from anesthesia or regarded as unreliable for follow-up.
We perform one-stage surgery, except in the case of very large and aggressive cholesteatomas, uncontrolled stapes cholesteatomas, infected cholesteatomas, large bony defects, mucosal inflammation, and poor middle ear ventilation.
The CWU technique also requires good-quality imaging follow-up. After cholesteatoma surgery, patients undergo an MRI exam at 12 months. If residual or recurrent cholesteatoma is suspected, a CT scan is performed. In the future, systematic MRI will probably replace the second-look procedure.
Revision surgery is performed in cases of functional failure, residual cholesteatoma suspected on follow-up CT scan or MRI, and recurrent cholesteatoma.
For further follow-up, an MRI exam is performed once a year for 5 years, especially in children.
Management of Controlled Posterior or Posterior Attic Retraction Pockets
Tympanomeatal Flap Incision
For retraction pockets, the meatal skin flap length must be at least 8–10 mm.
A retraction pocket with little epitympanic erosion can be managed using a transmeatal approach, with or without extended tympanoatticotomy.

Fig. 6.8
Fibrous Annulus Dislocation
With a needle or sickle knife, the fibrous annulus is dislocated from its sulcus, beginning at the inferior level where the tympanic cavity is aerated.
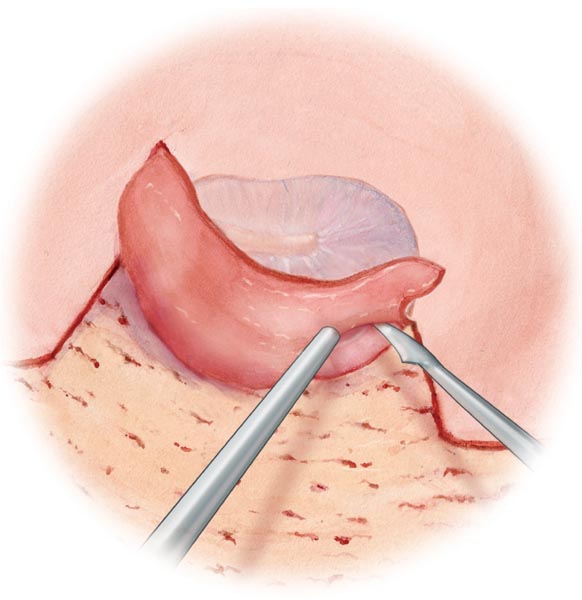
Fig. 6.9
Tympanic Membrane Dislocation
If the opening is large enough, a flap knife or dissector-elevator is inserted and the retraction pocket is slowly dissected and pushed out with the dissector-elevator. Sometimes, it requires use of a longer instrument called a meatus dissector-elevator.
Epidermic dissection of fragile structures, such as the incus, stapes superstructure, footplates, and chorda tympani, is required and should be carefully performed (see Hypotympanic, Protympanic, and Mesotympanic Cholesteatoma, p. 122).
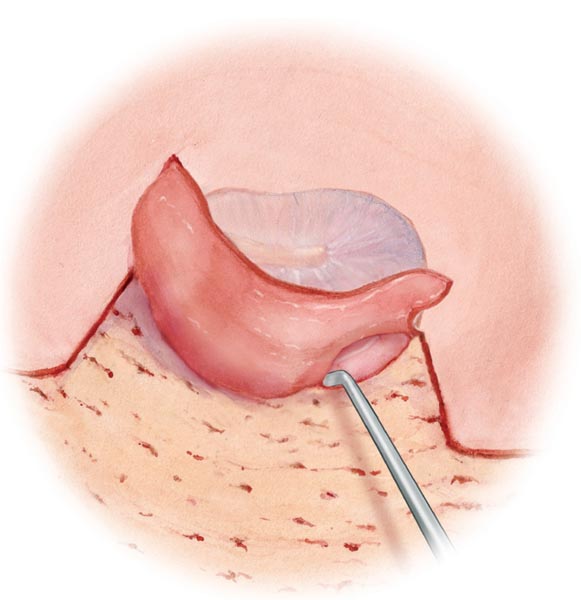
Fig. 6.10
Posterior Tympanoatticotomy
Depending on the extension of the retraction pocket, a posterior tympanoatticotomy is performed with a chisel or curette.
The tympanoatticotomy location allows different tympanic cavity approaches. Posterior tympanoatticotomy is the most common opening technique. It is used for middle ear exploration, ossiculoplasty with intact tympanic membrane, stapes surgery, and management of pathologies of the posterior tympanum
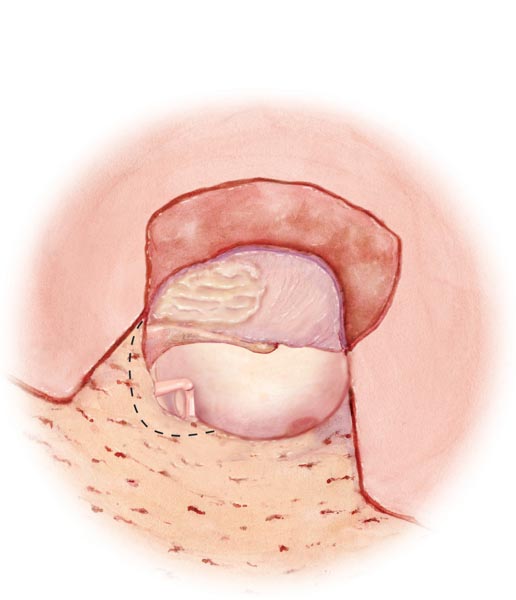
Fig. 6.11
Uncontrolled Extension
In the case of uncontrolled extension of a cholesteatoma to the facial recess and sinus tympani, a posterior tympanotomy is performed (see Posterior Tympanotomy, p. 119).
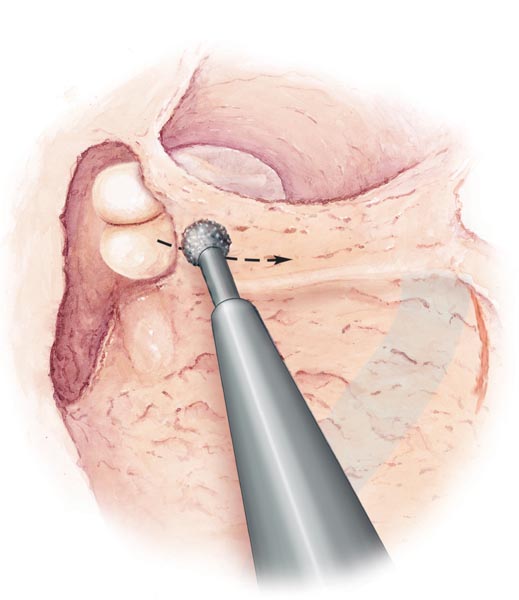
Fig. 6.12
Tip: Enter the middle ear cavity where the tympanic membrane is not retracted, but aerated, and slowly push out the retraction pocket to prevent tearing. Try to preserve the integrity of the tympanic membrane and also ensure that residual epithelium is not left behind. When the round window niche is recognized, proceed down to the pyramid and oval window. This can be checked using Zini mirrors or specially adapted otoendoscopes. If in doubt, perform a mastoid approach. Posterior tympanoatticotomy can also be extended to anterior tympanoatticotomy and/or inferior tympanotomy, if there is any pathological extension. If a drill is used for the tympanoatticotomy, remove the final bony overhang with a curette to avoid ossicular chain damage.
Cartilage–Perichondium Graft
The tympanic membrane is repaired using a tragal cartilage–perichondrium graft covering at least the posterior quadrants, the retracted tympanic membrane surface, and the bony wall defect (see Cartilage Tympanoplasty, p. 61).
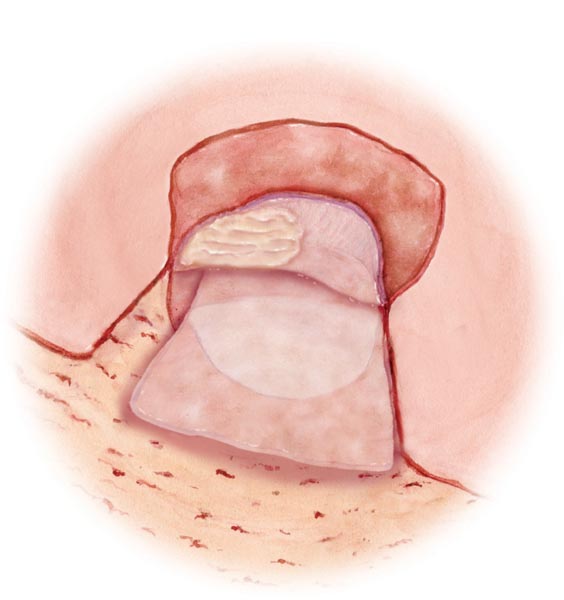
Fig. 6.13
Tip: Do not forget to check the integrity of the ossicular chain and repair it if necessary.
Management of Controlled Anterior Attic Retraction Pockets
Tympanomeatal Incision
The superior lateral skin incision is extended to the anterior canal wall several millimeters above the retraction pocket border. An anterior tympanoatticotomy is performed through a transmeatal approach using a small curette.
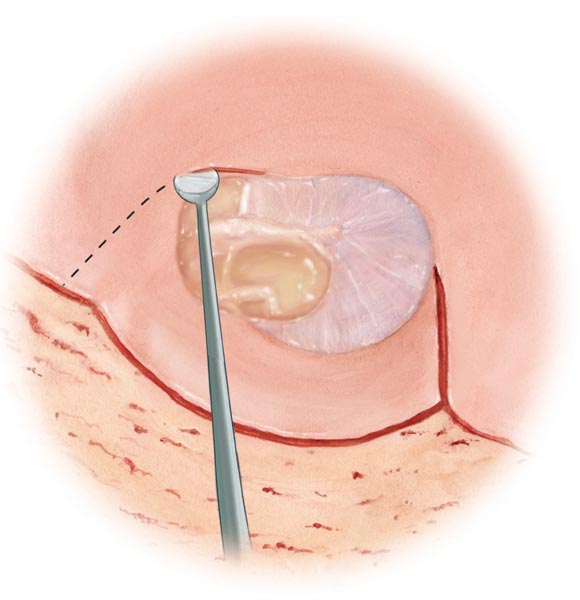
Fig. 6.14
Posterior Epitympanotomy
If there is any doubt regarding the presence of epithelium on the malleus head or cholesteatoma in the anterior epitympanum, a posterior epitympanotomy should be performed through a mastoidectomy (see Posterior Epitympanotomy, p. 117).
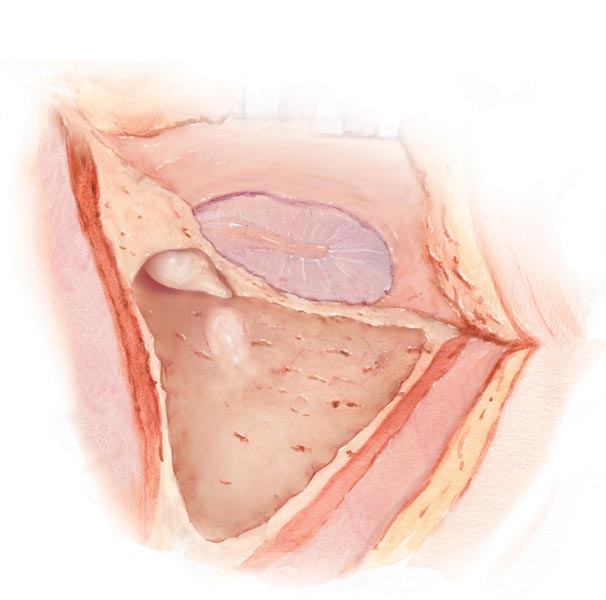
Fig. 6.15
The incus is removed and the malleus head cut. The cog (bony crest between the anterior and posterior epitympanum) is then removed using a diamond burr to open the anterior epitympanum and clean it.
The retraction pocket is pushed out from the epitympanic area to the external auditory canal using the dissector-elevator with or without a soaked cotton ball.
Tip: Extensive tympanoatticotomy should be avoided and a transmastoid approach should be chosen instead. If tympanoatticotomy is performed with a drill, do not touch the ossicular chain. In anterior tympanotomy (pretubal cells), be careful of the facial nerve and geniculate ganglion.
Transmastoid Approaches
Mastoidectomy
A mastoidectomy is indicated as a first-line approach for other middle ear pathologies, such as acute mastoiditis and meningoencephalic herniation into the mastoid and middle ear, as well as cochlear implantation.
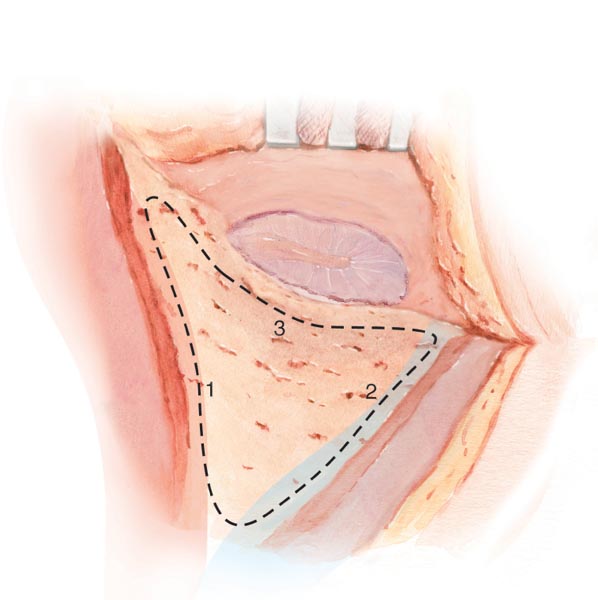
Fig. 6.16
Mastoid Landmark Identification
When the mastoid cortex is exposed, drilling with a large cutting burr should be started along the temporal line in an anteroposterior direction (1) to identify the middle fossa plate, followed by a posterior line to mark the sigmoid sinus (2). Finally, a third line is drilled just behind the posterior wall of the external auditory canal (3).
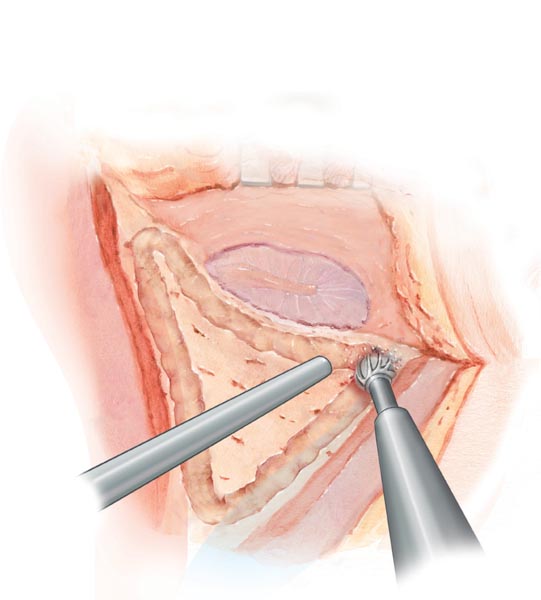
Fig. 6.17
Tip: Structures can be easily identified. The temporal plate is pink with small vessels, and the sigmoid sinus is blue. Vision should be adjusted to be parallel to the posterior wall of the external auditory canal to estimate its thickness and axis. Burr movements should be parallel to important structures. It is better to enlarge the mastoidectomy rather than drill a deep narrow hole.
Opening the Antrum
The next step is to find the antrum, which is situated between the posterosuperior angle of the external auditory canal and the anterior part of the temporal plate.
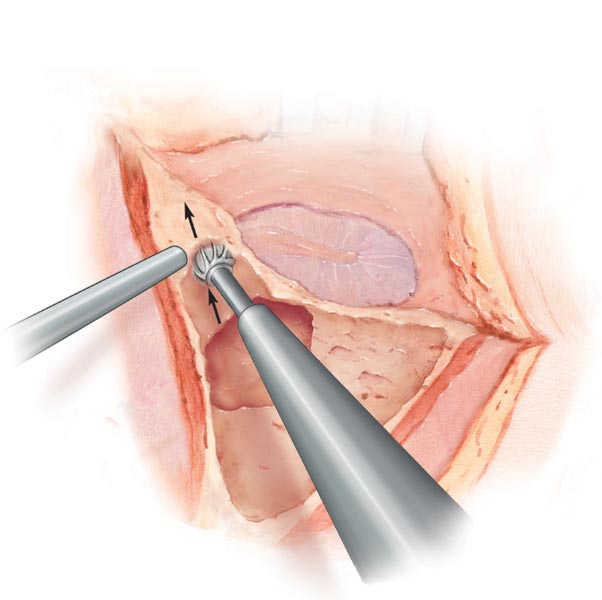
Fig. 6.18
Tip: The middle fossa plate may be situated low, hampering easy access to the antrum. The temporal plate and posterior bony wall should be thinned as much as possible. Significant temporal plate and external auditory canal defects should be fixed with bone pâté.
Opening of the Aditus
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


