Chapter 10
MANAGEMENT OF PATIENTS WITH POLYTRAUMA

Treating polytraumatized patients can be extremely challenging, requiring rapid and efficient collaboration of multiple specialists and paramedical personnel (e.g., nurses, technicians, emergency physicians, surgeons, radiologists, anesthesiologists, operating room personnel, even interpreters).
PEARL… Emergency medical technicians, police, and fire fighters often provide critical details of the injury and past medical history. They also help to preserve the integrity of evidence that might later be used in court.
In the initial phase of emergency medical care, the visual system commonly has low priority, but loss of vision can significantly diminish the quality of life for the otherwise rehabilitated patient and may result in the most devastating long-term disability.1
EPIDEMIOLOGY
A retrospective analysis1 of 1119 cases from a major hospital over a 7-year period (Fig. 10–1) found the following:
• age ranged from 15 to 90 years;
• 80% of the patients were male;
• 16% suffered ocular or adnexal injuries and 23% of these patients died;
• 29% had facial injuries, of which 55% were ocular injuries; and
• 1.2% of injuries resulted in vision less than 20/200.
Significant eye injury was statistically associated with the following:
• driving a motor vehicle;
• age younger than 50 years;
• male sex;
• associated basal skull fracture;
• orbital fracture; and
• lid laceration or superficial eye injury.
Of the patients with the most severe injuries:
• 0.8% had open globe injuries;
• 1.9% had optic nerve trauma, half of whom had vision less than 20/200; and
• 9.2% had orbital fracture.
In another study, among 6313 patients with major injuries admitted to a level I trauma facility over a 4-year period, 14% were found to have concomitant eye injury, most commonly eye/adnexa contusion (67%), adnexal lacerations (27%), and open globe injury (4%).2
INITIAL ASSESSMENT
The initial steps are based on the general principles of advanced trauma life support.a
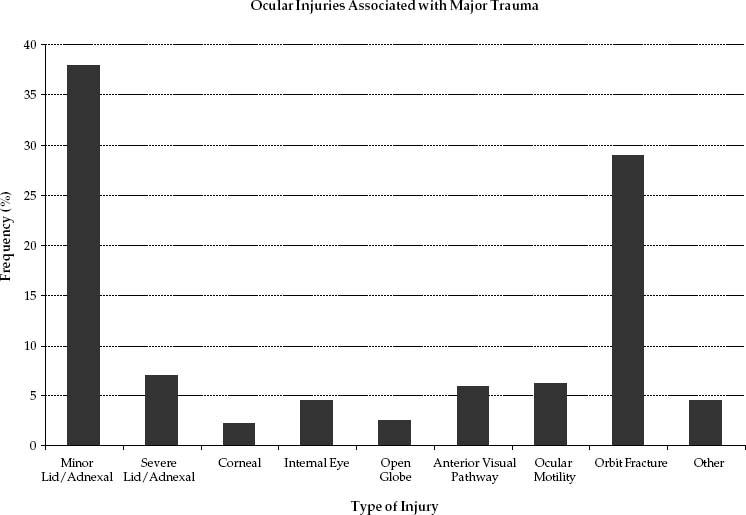
FIGURE 10–1 Ocular injuries associated with major trauma. (Adapted from Poon A, McCluskey PJ, Hill DA. Eye injuries in patients with major trauma. J Trauma. 1999;46:494–499. Reprinted by permission from Lippincott Williams … Wilkins.)
PEARL… In many cases, it is helpful for the ophthalmologist to be present in the ER or trauma room to try to protect the eyes during manipulations of the mouth, nose, and trachea. Emergency ocular problems (e.g., chemical burn, central retinal artery occlusion, open globes, retrobulbar hemorrhage) must also be addressed early.
When possible, an initial assessment of the vision should be performed, although altered mental status as a result of intracranial trauma or the use of analgesia or anesthesia may prevent this. The miotic effect of narcotic agents can hinder the examination of the pupils and the retina.
PEARL… In patients with severe intracranial injuries in whom changes in pupil size and reactivity may presage impending herniation and the need for immediate neurosurgical intervention, the integrity of the pupil (i.e., no pharmacologic dilation) is more important than the information provided by dilated-pupil IBO.
Finally, urgent ophthalmic problems should be assessed; in most cases, the initial triage is possible using only a penlight examination. The eye’s repair often has to be coordinated with other surgical interventions (e.g., an open globe should be closed before orbital surgery is performed; see Chapter 12).
Ocular conditions requiring immediate evaluation and/or intervention include:
• chemical burn (see Chapter 11) and, to a lesser extent,
• retrobulbar hemorrhage (see Chapter 12) and
• open globe injury (see Chapter 9).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


