Purpose
To report the efficacy of laser photocoagulation in treating idiopathic (primary) retinal vasoproliferative tumors.
Design
Retrospective noncomparative interventional case series.
Patients and Method
Thirty eyes of 30 patients (22 women and 8 men) with retinal vasoproliferative tumors. Main outcome measures were best-corrected visual acuity (BCVA), presence of retinal hard exudates, retinal detachment (RD), cystoid macular edema (CME), and epiretinal membrane (ERM). Laser photocoagulation was performed at the slit lamp or during pars plana vitrectomy for telangiectasia visible at the retinal vasoproliferative tumors surface.
Results
Fifteen eyes were treated with slit-lamp laser. Mean follow-up was 36.5 months (range 7 months to 11 years). Mean BCVA increased from 20/40 to 20/32 at the end of the follow-up. Hard exudates and CME regressed completely in 15 of 15 and 5 of 6 eyes, respectively. Fifteen eyes underwent vitrectomy owing to the presence of ERM (10 eyes), large exudative RD (4 eyes), or vitreous hemorrhage (1 eye). Mean follow-up was 24 months (9 months to 3.5 years). Mean BCVA increased from 20/125 to 20/40 at the end of the follow-up. No vision loss occurred. The retina reattached in all cases. Hard exudates regressed completely in 14 of 15 eyes and decreased significantly in 1. Postoperative complications were rhegmatogenous RD in 2 eyes, successfully reattached after additional surgery.
Conclusion
Selective laser photocoagulation of retinal telangiectasia at the retinal vasoproliferative tumors’ surface induced the regression of retinal exudation. Slit-lamp laser photocoagulation was sufficient in half of the cases. In more severe conditions, direct endolaser photocoagulation of the telangiectasia was required.
Retinal vasoproliferative tumors are a rare benign condition characterized by the presence of a peripheral retinal solid mass of unknown origin, associated with peripheral retinal telangiectasia, which in most cases leads to subretinal exudation. The condition’s clinical features have been clearly described in an extensive review of 103 cases by Shields and associates, who coined the name “vasoproliferative retinal tumors.” Treatment modalities are still controversial. Several methods have been proposed, most of them relying on the use of cryotherapy, laser photocoagulation, and also plaque radiotherapy. We report here our experience in the treatment of 30 eyes with retinal vasoproliferative tumors using either slit-lamp laser or endolaser photocoagulation.
Patients and Methods
We retrospectively reviewed the medical records of 30 consecutive patients who were referred for a peripheral exudative retinal mass in the Ophthalmology Department at Lariboisière Hospital (Paris, France) and who were diagnosed with retinal vasoproliferative tumors between 2000 and 2011. Patients (22 women and 8 men) were aged from 10 to 70 years (mean: 40.6 years). They all had some degree of vision impairment. This retrospective study adhered to the principles of the Declaration of Helsinki. The Ethics Committee of the French Society of Ophthalmology did not find any challenge against the medical and scientific rules of ethics, as accepted in France.
Each patient underwent a comprehensive ocular examination, including the best-corrected visual acuity (BCVA), intraocular pressure, and anterior segment examination with a careful evaluation of the ocular inflammation, and 3-mirror or wide-field contact fundus lens biomicroscopy for examination of the peripheral retina. Color photographs and fluorescein angiography of the posterior pole and peripheral retina (TCR 50; Topcon, Tokyo Japan) were performed at the initial examination and during the follow-up. Optical coherence tomography (OCT) of the macula was recorded on Stratus or Cirrus (Carl Zeiss Meditec, Dublin, California, USA) and Spectralis OCT (Heidelberg Engineering GmbH, Heidelberg, Germany).
The features taken into account included the presence of cells in the vitreous, intraretinal or subretinal hard exudates, serous retinal detachment (SRD), cystoid macular edema (CME), and epiretinal membrane (ERM), assessed on fluorescein angiography and OCT.
Inclusion and Exclusion Criteria
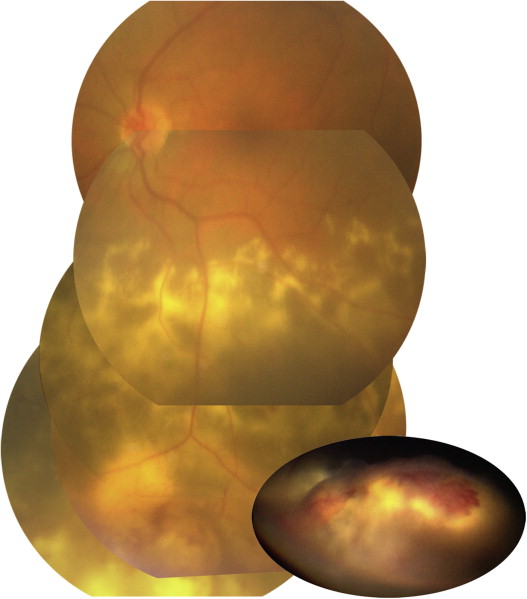
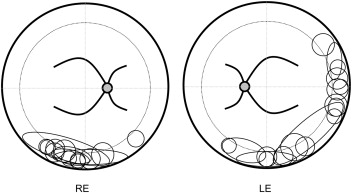
Although retinal vasoproliferative tumors have no pathognomonic clinical characteristics, the diagnosis was based on the presence of a solid yellowish peripheral retinal mass overlaid by retinal telangiectasia and surrounded by subretinal hard exudates and SRD ( Figure 1 ). On fluorescein angiography, early frames centered on the peripheral mass showed the filling of an irregular retinal vascular network consisting of telangiectatic capillaries with progressive dye leakage ( Figures 4 and 5 ) and late frames were recorded on the macula to assess the possible presence of CME. These features could be associated with ERM and CME. In all 30 patients, the yellowish solid mass was located in the temporal, temporal inferior, or inferior retinal periphery ( Figure 2 ). In 14 out of the 30 patients, ultrasonography had been performed to rule out a malignant tumor.
We excluded patients who presented with a coarse capillary network suggestive of Coats disease, near the lesion or somewhere else in the fundus; patients with large feeder vessels suggestive of von Hippel–Lindau disease or family history of this disease; and other preexisting diseases such as intermediate uveitis, toxocariosis, retinitis pigmentosa, neurofibromatosis, chronic retinal detachment (RD), or history of scleral buckling in RD.
We therefore only reported the outcome of patients with idiopathic or primary retinal vasoproliferative tumors after laser treatment.
Treatment
Patients were divided into 2 groups, depending on the treatment received: slit-lamp laser or endolaser photocoagulation.
Slit-Lamp Laser Photocoagulation
Fifteen out of our 30 patients were treated only with slit-lamp 532 nm laser photocoagulation. The parameters used were as follows: duration, 0.3–0.5 seconds (and even 1 second in some cases); intensity, 200–500 mw; and spot size, 50–100 μm. The beam was focused on the small vessels and telangiectasia visible at the tumor mass surface. Despite the intensity of the laser burns, the treatment was usually painless, probably owing to the thickness of the tumor or to the underlying hard exudates, which prevented the laser burns from reaching the choroid. Most often, a single slit-lamp laser session was not sufficient to completely eradicate the vascular anomalies. Patients received 2–8 laser photocoagulation sessions within a few weeks to ensure the closure of all telangiectasia, which could have reopened after a previous session. They were followed up on the basis of a weekly examination during the first month until telangiectasia were definitely closed or the eye was assigned to retreatment.
Endolaser Photocoagulation
In the 15 remaining patients, laser treatment was performed during 3-port pars plana vitrectomy, because slit-lamp laser was ineffective to permanently close the telangiectasia owing to lens opacities and haziness of the peripheral vitreous in 2 cases, because of the presence of an ERM in 9 cases, because of a vitreous hemorrhage in 1 case, and because of an extensive RD complicated by an ERM or severe vitreous haze in the 3 remaining cases. The presence of a macular ERM, which contributed to the vision loss, prompted us to perform endolaser, together with the vitrectomy, to treat the telangiectasia.
Surgery consisted of 3-port pars plana vitrectomy (20 G for the first cases and 25 G for the last ones) combined with wide-angle viewing system. An ERM was removed in 9 cases. An endocular 532 nm laser (Eyelit; Alcon, Fort Worth, Texas, USA) was used via an illuminating laser probe to coagulate peripheral telangiectasia under scleral depression. Long-duration and high-intensity laser burns were delivered directly to the telangiectasia and afferent vessels. Because of the close proximity between the tip of the laser probe and the retina, it was possible to deliver a high laser energy, which resulted in telangiectasia closure in a single treatment session. In a single patient in whom the amount of exudates in the subretinal space was especially massive, a trans-scleral drainage of the subretinal fluid was performed to evacuate, as much as possible, the exudates.
Results
Slit-Lamp Laser Photocoagulation
In this group of 15 patients, the mean follow-up was 36.5 months (range 7–132 months). Initial BCVA ranged from 20/20 to counting fingers (median: 20/40). Six patients had a cystoid macular edema, and 2 had a massive intraretinal and subretinal accumulation of hard exudates in the macula. All the patients had peripheral exudates and subretinal fluid around the tumor. At 6 months, the visual acuity ranged from 20/20 to 20/500. Median final visual acuity was 20/32 (20/20–20/500). The macular edema and exudates regressed in all patients ( Figure 3 ), except 1 in whom the macular edema persisted after exudate resorption. In 2 eyes, a subretinal macular fibrosis appeared after hard exudate resorption. Peripheral exudates and the subretinal fluid regressed in all cases.
Endolaser Photocoagulation
In this group of 15 patients, the mean follow-up was 23.8 months (range 9–43 months). Initial BCVA ranged from 20/40 to counting fingers (median: 20/125). Five eyes had a cystoid macular edema and extensive subretinal exudates were present in all cases, reaching the macula in 8 eyes. All eyes exhibited evidence of serous retinal detachment. An ERM was also present in 9 eyes. One eye had a vitreous hemorrhage. At 6 months, the median visual acuity was 20/40 (20/20 to counting fingers). No vision worsening was observed in any eye. The subretinal fluid and exudates completely regressed in 14 out of the 15 patients ( Figures 4 and 5 ). In the remaining eye, the exudates only partially but significantly regressed at the end of a 9-month follow-up. The CME regressed in all cases. The tumor itself became white after laser treatment (by slit-lamp or endolaser), but did not disappear.



