Chapter 26
MANAGEMENT OF EYES WITH PERFORATING INJURY

The Ocular Trauma Classification Group classified perforating ocular injuries as type D, typically involving zone III (see Chapters 1 and 2). These injuries are usually1–11 associated with a worse outcomea than contusions, IOFBs and penetrating trauma, and they can occasionally be as serious as ruptures. This chapter describes the unique aspects of treating eyes with injuries involving both entrance and exit wounds.
EPIDEMIOLOGY
• The incidence of perforating injuries varies widely and is reported between 7% and 31%, depending on study criteria and terminology.1–5,7,12
 Among all injured eyes undergoing vitreoretinal surgery, the incidence decreases to 4–10%.2,3,7
Among all injured eyes undergoing vitreoretinal surgery, the incidence decreases to 4–10%.2,3,7
 If limited to injuries caused by high-speed projectiles, (e.g., industrial nail guns,13 BB guns,14,15 and shotguns,6,10,16,17), the incidence rises to 50–92%.
If limited to injuries caused by high-speed projectiles, (e.g., industrial nail guns,13 BB guns,14,15 and shotguns,6,10,16,17), the incidence rises to 50–92%.
 The rate is 0.075% among retrobulbar injections.18
The rate is 0.075% among retrobulbar injections.18
 Missiles are the cause in three fourths of eyes.19,20
Missiles are the cause in three fourths of eyes.19,20
The following is the epidemiological information found by the USEIR.
Rate of perforating injury among all serious injuries: 3%.
Rate of perforating injury among open globe injuries: 5%.
Age (years):
• range: 2–77;
• average: 24.
Sex: 87% male.
Place of injury:
• home: 40%;
• industrial premises: 18%;
• recreation and sport: 15%;
• street and highway: 9%;
• public building: 4%.
Source of injury:
• gunshot: 38%;
• various sharp objects: 18%;
• BB/pellet gun: 17%;
• hammering on metal: 9%;
• various blunt objects: 4%;
• MVC: 3%;
• explosion: 2%.
Rate of corneo/scleral perforationsb: 53%.
Rate of sclero/scleral perforations: 47%.
The typical perforating injury is caused by:
• a high-speed projectile or missile (e.g., BB or shotgun pellet); or, less commonly,
• a sharp object (e.g., blade, nail, broken glass).
Most projectiles are blunt; some,19 but not all,3 studies report a worse prognosis associated with projectile injuries (see Table 26–1 for the muzzle velocities of projectiles causing perforating trauma).
PEARL… Blunt objects (e.g., BB or shotgun pellet) require higher velocity (i.e., kinetic energy34) to enter (rupture/perforate) the globe. The energy is absorbed by the eye, causing significant damage (see Chapters 1 and 3).
A sharp object is able to perforate the eye at a much lower velocity, often causing less severe coincidental damage18,20,21 unless resulting in retinal detachment, submacular hemorrhage, direct macular or optic nerve injury, or multiple posterior exit wounds (“sewing machine injury”22).
Nails fired from an industrial nail gunc are sharp projectiles.d There are limited data regarding their prognosis.13
The damage occurring at the time of a perforating injury is compounded by scarring (i.e., consequences of the eye’s own healing response; see Chapter 8),23–26 which is frequently far more deleterious to the eye than the initial trauma.
Contracting membranes may be present as early as 6 hours after injury.26 Several factors, including blood28–30,e and lens injury,31,32 may contribute to the development of tractional retinal detachment.
Fibrosis, the first step in PVR, begins at the scleral wound(s). The amount of new collagen increases most dramatically between 14 and 30 days, especially in the presence of autologous blood.33,34 The tract connecting the entry and exit wounds becomes a scaffold for fibroblast proliferation as early as 4 days after injury,35 leading to anteroposterior traction.36
| Projectile | Muzzle Velocity (m/sec) |
|---|---|
| Shotgun pellet16 | 243 |
| BB (pump-action rifle)71 | 213 |
| Nail (industrial nail gun)13 | 125 |
| BB (spring-loaded rifle)16 | 91 |
*The velocity of a projectile is highest immediately upon being fired (muzzle velocity) and is progressively slowed by air resistance. As a reference, the estimated velocity of a BB necessary to perforate an eye consistently is 73 m/sec for the rabbit, 103 m/sec for the human, and 113 m/sec for the dog.27 (It should be noted, however, that there is significant individual variability in these measurements, as BBs from a spring-loaded rifle [muzzle velocity 91 m/sec] have been documented to cause perforating injuries.16) Generally, shotgun pellets cause more severe damage than BBs because of their higher velocities. However, newer pump-action BB rifles achieve muzzle velocities approaching those of shotguns, and devastating injuries may ensue (e.g., perforating the cornea, lens, vitreous, and optic disk and coming to rest in the substance of the optic nerve 2 mm posterior to the lamina cribrosa71). A shotgun pellet may also fragment upon striking the anterior surface of the eye, resulting in multiple exit wounds.56,57
PEARL… The two most important factors in PVR development appear to be vitreous hemorrhage and vitreous incarceration in the wound37; injury to the lens, vitreous, and/or ciliary epithelium appears to accelerate this process26.
Traumatic vitreopathyf may make visualization more difficult; the developing partial posterior vitreous separation accentuates the anteroposterior traction between the exit wound and the vitreous base.39
PITFALL
In the previtrectomy era, the majority of eyes with perforating trauma eventually lost light perception, became phthisical, or required enucleation, typically because of irreparable retinal detachment and hypotony.9,16,40,41
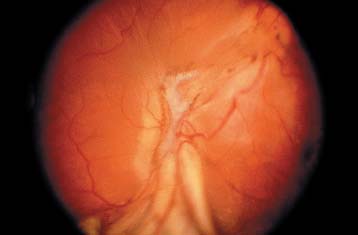
FIGURE 26–1 Dart injury with a posterior exit wound along the inferior vascular arcade. The patient had minimal vitreous hemorrhage, allowing direct visualization of the extent of posterior segment damage. Vision was hand motions due to development of a retinal detachment with PVR. Vitrectomy was performed with retinectomy of the incarcerated tissue, laser photocoagulation, and placement of silicone oil. Final vision was 5/200.

FIGURE 26–2 B-scan echogram suggesting a subtle defect in the posterior sclera as a result of an assault with an ice pick. The area of abnormality is marked by the presence of retinal and vitreous incarceration into the scleral wound. Presence of an exit wound was confirmed at the time of vitrectomy, and the incarcerated tissue was removed.
SURGICAL TREATMENT
Vitrectomy
Timely vitrectomy1,9,26,35,39,42,51 serves many purposes, including:
• removal of:
 clotted hyphema;
clotted hyphema;
 injured lens;
injured lens;
 vitreous hemorrhage; and
vitreous hemorrhage; and
 IOFBs; as well as
IOFBs; as well as
treatment of all treatable lesions (see Figs. 26–1 through 26–4) in the posterior segment.
PEARL… Vitrectomy improves the prognosis for perforating eye injuries when compared with the natural history.52
A meta-analysis of published reports1,5,11,13,15,17,19,21,22,53–58 on eyes undergoing vitrectomy for perforating trauma (excluded were series not satisfying both criteria2,3,4,6,7,11,52) showed anatomicalg
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


