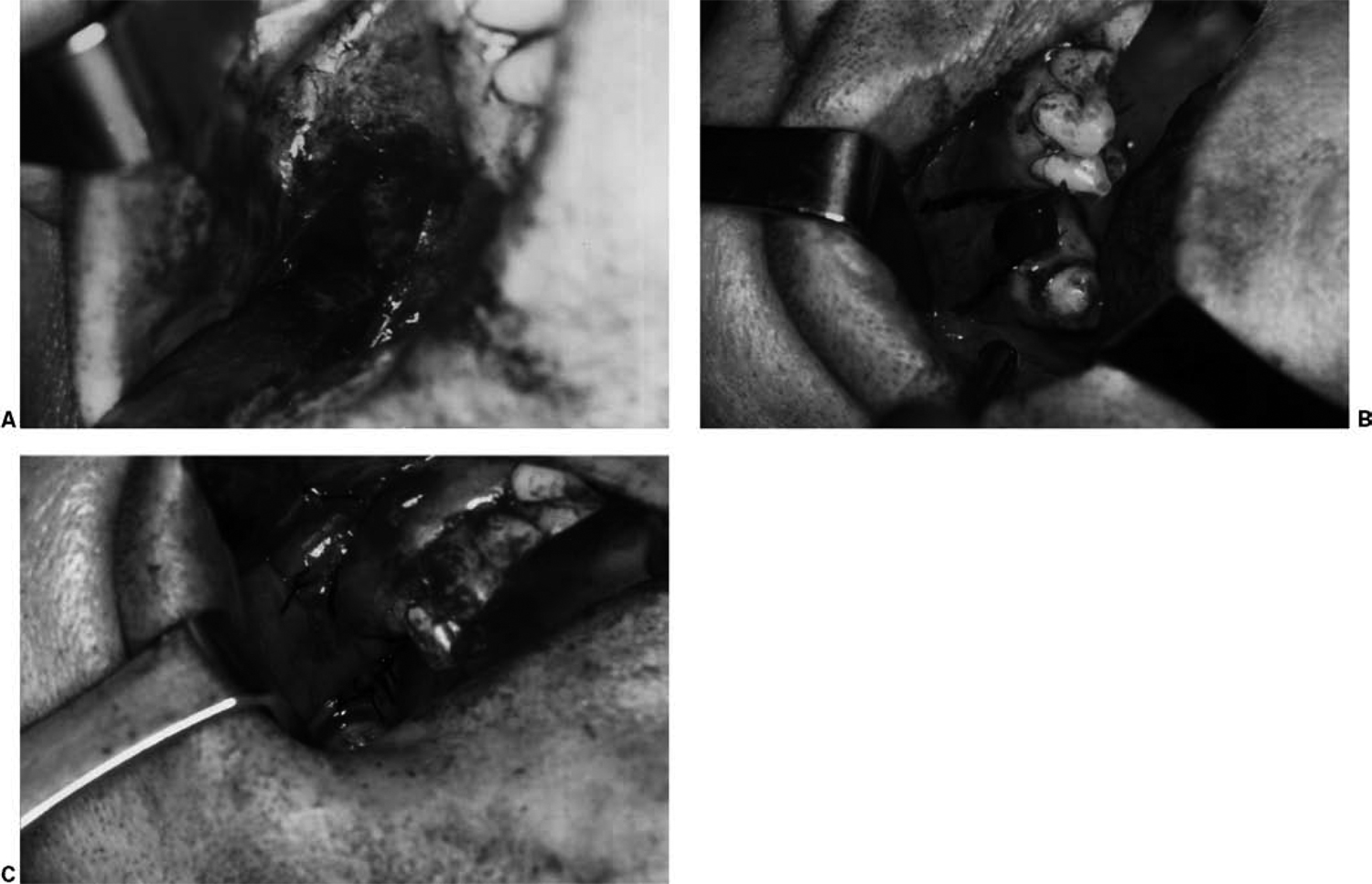
1 Management of Benign Oral Cavity Lesions A permanent communication between the maxillary sinus and the oral cavity may result following the extraction of a maxillary bicuspid, or molar tooth. An attempt is often made at the time of the removal of the tooth to close a recognized perforation into the sinus by the dental surgeon, which may or may not be successful. Usually the communication goes unrecognized, and a permanent tract develops, with the patient presenting with a history of fluids draining through the nose while eating. One or several attempts at closure of the fistula ensue, which, again, may or may not be successful. The root cause of the fistula forming and persisting after an attempt has been made at repair is the presence of chronic maxillary sinus disease, which uses the tract for dependent drainage. After a preliminary course of antral irrigations and antibiotic therapy, a computed tomography (CT) scan should be taken, which will generally reveal diffuse mucosal thickening, or total opacification of the maxillary sinus, often with adjacent disease in the ethmoid sinus. A foreign body from previous dental manipulation may also be identified in the sinus. It has been the author’s experience that endoscopic sinus surgery directed at the middle meatus is insufficient to resolve the antral infection and permit sufficient removal of the irreversibly damaged mucosa necessary for the successful closure of the fistula. The author favors an approach to the antrum through the canine fossa and the use of a buccal mucosa advancement flap to close the fistula (Fig. 1.1). The procedure consists of coring out the epithelium of the fistula tract with a no. 11 blade and curetting the granulation tissue present on the adjacent bone. If one side of the fistula is not covered by bone, but by the root of an adjacent tooth, that tooth should be extracted; otherwise, complete epithelial closure over the defect will not be accomplished. Following this, two slightly divergent vertical incisions are made across the alveolus toward the cheek. A conventional transverse Caldwell-Luc incision would eliminate the ability to create this buccal advancement flap and should not be attempted. The flap to be elevated consists of mucoperiosteum and will not advance until the periosteum is incised on its undersurface with either a no. 15 blade or an iris scissors. The flap will then be freely mobile and is advanced and sutured to the palatal mucosal with interrupted 4–0 Vicryl sutures. Before the actual fistula closure is performed, another vertical incision is made along the long axis of the canine tooth, and the mucoperiosteum over the canine fossa is elevated. An opening into the antrum is made with a mallet and gouge and enlarged with a Kerrison-type punch forceps. This permits removal of the diseased mucosa directly and with endoscopic guidance. Another antrostomy is created in the inferior meatus, which facilitates cleansing of the sinus and will provide dependent drainage for the antrum. This incision is also closed with 4–0 Vicryl sutures. The key to oroantral fistula repair is removal of the diseased mucosa of the antrum, as a fistula does not develop following dental extraction when a healthy maxillary sinus is present. Fig. 1.1 (A–C) Repair of oroantral fistula. Fig. 1.2 (A, B) Excision of dentoalveolar lesion. In patients with disease involving the dental alveolus, by extension downward from a benign maxillary sinus tumor, or inflammatory lesion, or by growth upward of a dental cyst or tumor into the antrum, complete exposure of the lesion and secure closure of the incision cannot be accomplished by the standard transverse Caldwell-Luc incision. Excision of the lesion will include removal of a portion of the alveolus and the lateral wall of the antrum. An incision not supported by bone invites the postoperative formation of a fistula. If the extraction of a tooth is necessary, the opening in the alveolus cannot be closed primarily with such an incision. The use of a gingival flap obviates these difficulties (Fig. 1.2). This is created by incising the attached gingival with a no. 15 blade along the necks of the posterior maxillary teeth in the gingival sulcus. Posteriorly, the incision is carried over the maxillary tuberosity. Anteriorly, a vertical incision is made in the long axis of the canine tooth. Using a Freer elevator, the entire gingival and alveolar mucosa and the mucoperiosteum over the lateral wall of the maxillary sinus are elevated readily. The bone over the lesion is removed to expose its extent. The lateral wall of the antrum adjacent to it is also removed sufficiently to determine the degree of involvement of the sinus. The lesion is then removed, and the bone about it is curetted. The gingival flap is returned and fixed with interdental sutures of 4–0 Vicryl. If the removal of a single or multiple teeth has been necessary, relaxing incisions are made similar to those described in the previous section, and the buccal mucosa is advanced and sutured to the palatal soft tissues. If the antral mucosa is healthy, it is left undisturbed, and a small temporary antrostomy is made in the inferior meatus for dependent drainage. This approach provides wide access for removal of alveolar-antral lesions and permits the primary closure of the incisions about the resulting defect. These lesions occur in the oral cavity on the gingiva and appear predominantly as broad-based reddish masses extending along the necks of several teeth. Occasionally, they are seen on the edentulous alveolus. They represent hyperplastic reparative growths composed of giant cells in a highly vascular stroma. Although histologically identical to the centrally occurring giant cell granuloma and tumor, they are self-limited and less destructive than their intraosseous counterparts and are not associated with hyperparathyroidism. These are completely benign soft tissue lesions, although they may cause minor bone erosion by compression. Treatment is by simple excision with a sickle knife (no. 12 blade), removing the marginal gingiva and the interdental papillae, with healing by secondary intention. With recurrent lesions, it may be necessary to extract the involved teeth, as the granuloma may be present in the periodontal membrane space. Clinically, it must be differentiated from the pregnancy tumor, which has an identical appearance and develops in response to elevated estrogen levels in gravid women. Many of these lesions spontaneously involute postpartum. However, surgery, which should be performed in the second trimester, may be indicated if the lesion persistently bleeds. This inflammatory lesion develops on the hard palate of full denture wearers and presents as a large, but well-circumscribed, irregularly elevated papillary and nodular area (Fig. 1.3
Oroantral Fistula

Dentoalveolar Lesions
Hyperplastic Lesions
Giant Cell Granuloma
Palatal Papillary Hyperplasia
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


