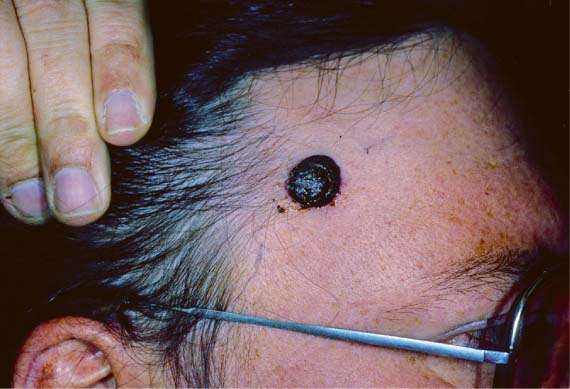
40 A 46-year-old white man presented with a rapidly enlarging black lesion on the right temple. He did not have a personal or family history of dysplastic nevi or melanoma. Physical examination revealed a 2-cm black irregular mobile nodule on the right temple (Fig. 40.1). No palpable preauricular, postauricular, anterior, or posterior cervical lymphadenopathy was noted. He denies weight loss. The following lesions should be considered in a patient with suspected melanoma (including lentigo maligna and amelanotic melanoma): Benign lesions. Benign melanocytic nevus, dysplastic melanocytic nevus, seborrheic keratosis, lentigo simplex/solar lentigo Malignant lesions. Pigmented basal cell carcinoma, squamous cell carcinoma, Merkel cell carcinoma, atypical fibroxanthoma, cutaneous metastasis 1. Diagnostic features. The ABCD rule is useful in differentiating acquired nevi from melanoma: A, asymmetry; B, irregular border; C, variegated color; D, diameter greater than 6 mm. Lesions that satisfy one or more ABCD criteria should be considered for biopsy. Note that congenital nevi tend to be larger, and size is not helpful unless there has been a rapid increase. 2. Full skin examination and regional lymph node palpation are essential in any patient with suspected melanoma. 3. Patients with dysplastic nevi have a 2 to 12% increased lifetime risk of melanoma. Prophylactic removal of dysplastic nevi does not eliminate risk of developing melanoma but serves as a marker of increased risk. Excision of dysplastic nevi with moderate to severe atypia is advised. Given the location of this patient’s lesion, an excisional biopsy with 2-mm margins was performed and revealed a nodular proliferation of markedly atypical melanocytes extending to the deep dermis (Breslow thickness 3.3 mm, Clark level IV, nonulcerated). A properly performed biopsy is critical for accurate diagnosis of melanoma. In most cases this will entail an excisional biopsy; however, an incisional or punch biopsy can be performed on large lesions (>2 cm) or for those that would require elaborate reconstruction and planning. An incisional/punch biopsy should be performed on the most raised and the darkest portion of the lesion and should include full-thickness skin and subcutaneous fat. Excisional biopsy should be down to the level of the underlying fascia. For lentigo maligna, a Wood’s lamp may be helpful in delineating unclear borders of suspicious lesions. Fig. 40.1 Presenting lesion. As evidenced in the 2002 American Joint Committee on Cancer (AJCC) melanoma staging system (Table 40.1), Breslow thickness, the presence of ulceration, lymphatic invasion, and the presence of distal metastases are the most important prognostic indicators in primary cutaneous melanomas. Breslow thickness is measured from the granular layer of the epidermis to the deepest portion of the tumor. Clark level (level of dermal involvement) is often reported but is not of prognostic significance except in differentiating stage 1A and 1B melanomas. Malignant melanoma, 3.3-mm Breslow thickness, Clark level IV, nonulcerated
Malignant Melanoma
History
Differential Diagnosis—Key Points
Test Interpretation
Diagnosis
Medical Management
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


