10 Malformations
Indications
• Thornwaldt cyst and other cysts
• Choanal atresia
• Dysplasia of the nasal septum and conchae
• Osler disease
• Spontaneous dural fistula
• Meningoencephalocele
Principles
From a surgical point of view, congenital malformations of the head can be compared to anatomical abnormalities and be regarded as endoscopic targets if their repair is indicated. The guidelines for reconstructive measures are identical to those for injuries as described in Chapter 9 and for neoplasias or tumorlike lesions dealt with in Chapter 11. Their common concern is to keep the access portal as limited as possible but large enough to allow precise manipulations with special instruments under visual control. According to the surgeon’s skill and experience, a decision on either the endoscopic or a broader external approach must be based on the patient’s individual circumstances.
Operative Technique
Thornwaldt and Other Cysts
The typical congenital cyst at the upper dorsal wall of the pharynx can be appreciated as a round primordial cleft of varying depth with a mucosal cover and an internal cuboidal epithelium. It may also originate from Rathke’s pouch, which is the primordium of the anterior pituitary, lying immediately anterior to the buccopharyngeal membrane, arising as an outgrowth of the dorsal ectoderm of the mouth (Davies 1973; Toomey 1973).
Similar formations may occur in the tonsillar pouch. A cystectomy can easily be executed by endoscopic or microscopic transnasal marsupialization using laryngeal scissors (Fig. 10.1a, b) . Preoperative diagnosis must exclude a meningocele and a cystic craniopharyngioma by skull base imaging. Mucosal retention cysts of similar appearance may grow in persistent adenoids and at the choanae. Flanking septoplasty or posterior conchotomy will eventually facilitate the endoscopic exposure of the nasopharynx.
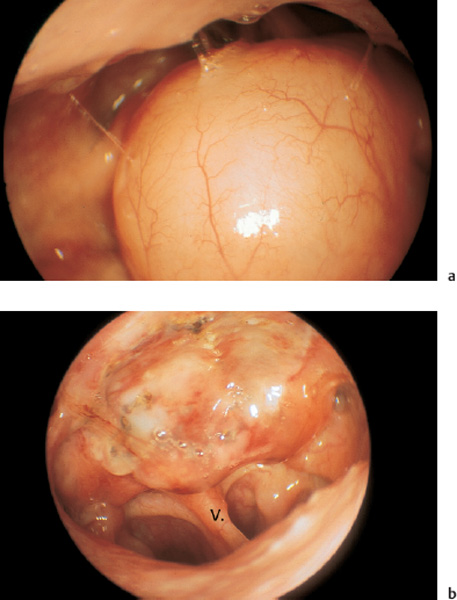
Fig. 10.1 a, b Congenital rhinopharyngeal cyst.
a Posterior aspect of a large cyst at the roof of the nasopharynx (90° telescope transorally introduced).
b The same aspect after endoscopic removal with a CO2 laser. V = nasal vomer.
Other cysts of embryological origin are found on the bottom of the common nasal meatus or in the maxillary sinus, sometimes containing a dental primordium (Fig. 10.2a, b).
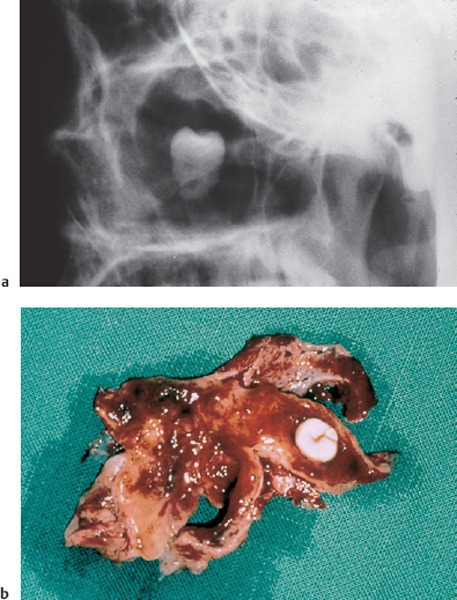
Fig. 10.2 a, b Dental primordium in the left maxillary cavity.
a Lateral view on the radiograph.
b The antral cyst with the retained tooth after transnasal removal.
Choanal Atresia
Congential nasopharyngeal partitions may be membranous, bony or partly membranous. Usually they are smaller than a normal choana.
Division of a choanal atresia in newborns and infants using the operating microscope and a carbon dioxide laser has proved to be very valuable (Wigand 1990). It is simple, but application of the beam to the correct point can be obstructed by the turbinates or septal spurs (Fig. 10.3a–c) . The nasopharynx should be protected with moistened cotton before coagulation is begun. Since the theoretically useful guidance of the penetration by a CAS modality is in most cases not attainable, the laser beam must be directed according to landmarks: It is kept close and parallel to the nasal septum and consequently in a sagittal plane. The level of the projected opening corresponds to that of the posterior tip of the inferior turbinate see Fig. 2.36). A reliable alternative is perforation of the bony choanal plate with a long-shafted diamond microdrill (Fig. 10.3c) . The new nasopharyngostomy may be stented with a Teflon tube of about 5 mm diameter for some days. This aid can prevent early stenosis by fibrin clots but will not necessarily prevent later narrowing by scar tissue. This rather primitive laser penetration is admittedly an emergency measure for newborns who cannot swallow without nasal respiration, to be repeated after some months or to be completed later by a plastic reconstruction of the choana.
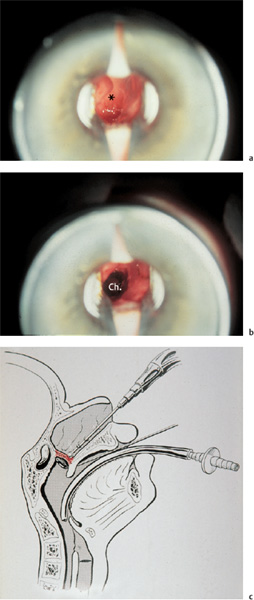
Fig. 10.3 a–c First-stage opening of a bilateral choanal atresia in the newborn.
a The transnasal endomicroscopic view of the choanal plate.
b The new window after fenestration with a CO2 laser.
c Transnasal drilling of the atresial plate (schematic drawing from Mündnich 1962).
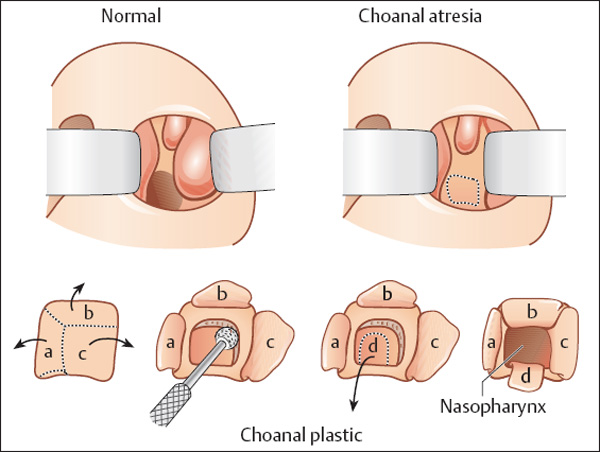
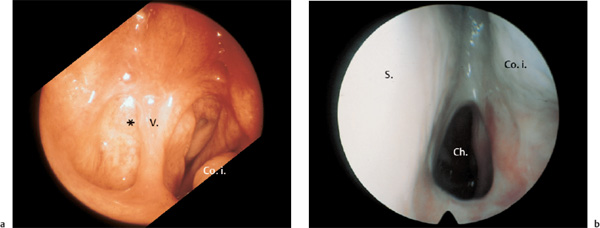
Fig. 10.5 a, b Unilateral choanal atresia in a 17-year-old girl.
a The retrograde transoral exposure of the bony plate (*) (90° telescope).
b New choana after plastic reconstruction (0° telescope).
Unilateral choanal atresia in adults allows a safer technique including plastic lining of the newly produced tunnel with a mucosal flap. After good exposure of the closed and mostly deformed choanal region using a self-retaining speculum and operating microscope, an angled incision of the overlying mucosa, forming an inverted L with the angle medially, is carried out, thus allowing a triangular flap to be swung laterally (Fig. 10.4). The underlying obstructive block of bone is then drilled, if necessarywith a supportive resection of the neighboring vomer utilizing a back-biting punch.
The pharyngeal mucosa covering the posterior surface of the atresial plate can now be inversely incised, if still in place, in order to form a caudally pedicled flap. After an adequate opening has been established, all mucosal flaps are swung into the new choana, and fixed with tissue adhesive or by simple stenting with a plastic tube of suitable diameter. Figure 10.5 a, b gives an example of a choanal reconstruction following this principle. Successful endoscopic management without prolonged stenting was reported for 40 children with 26 unilateral and 14 bilateral atresias (van den Abbeele et al. 2002) . Patency was defined as less than 50% restenosis (Schoem 2004). A literature review of various techniques and their complications has been given by Stamm (Stamm et al. 2000b).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


