Malar Fractures
Malar fractures usually occur as a result of direct trauma to the malar eminence (cheekbone). The malar bone fractures at its frontal, temporal, and maxillary attachments. The resulting fracture is often depressed and rotated.
39-1 Treatment of Malar Fractures
Indications
A depressed malar fracture with cosmetic deformity or functional consequence, such as diplopia, requires surgical intervention.
Preoperative Evaluation
Fracture step-offs can often be palpated along the inferior orbital rim and at the zygomatic frontal attachment. Infraorbital hypoesthesia may be present from injury to the infraorbital nerve. Pediatric low-dose radiation computed tomography (CT) of the facial bones is best to demonstrate the fracture and any associated injuries. Ophthalmologic evaluation should be obtained prior to surgical intervention. Fracture reduction should be carried out when the patient’s general condition is stable and the edema has subsided (usually 3–5 days).
Fixation of fractures should be accomplished with plating technology. Titanium and resorbable plating systems are now widely available. If titanium plates are used, there is some controversy over whether they need to be removed. Proponents of removal believe that plates should be removed after 2–3 months, once healing has occurred, to prevent plate migration or skeletal growth alterations. Some believe that children younger than 10 years of age should be managed utilizing either titanium plates with subsequent removal or resorbable plates. Those older than 10 years of age should be treated similarly to adults with titanium plates not requiring removal. Others believe that removal of titanium plates is not an issue and recommend removal only in cases of infection, hardware failure, or tooth bud injury.
In the absence of displacement or functional deficits, conservative management can be instituted with soft diet and observation.
Operative Technique
1. Malar fractures are best reduced in children utilizing general anesthesia.
2. Corneal protection must be employed by performing a tarsorrhaphy suture with a 6-0 nylon or Prolene (Ethicon) suture through the gray line of the lid margins.
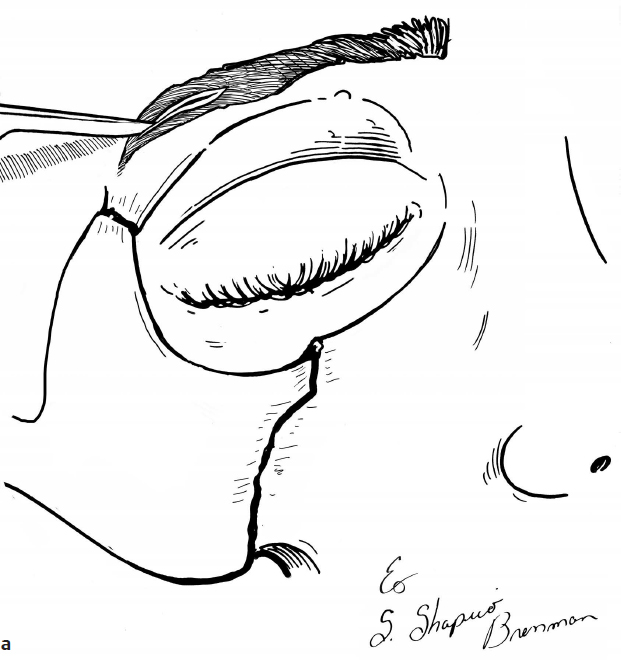
3. One percent lidocaine with 1:100,000 epinephrine is injected at the incision site to aid in hemostasis. No hair is shaved for the incision. The incision is made in the lateral eyebrow within the eyebrow itself paralleling and preserving the hair follicles (Fig. 39.1a). An upper blepharoplasty incision can also be employed to gain access to the lateral orbital rim as well (not shown).
4. For a subciliary approach, an incision is made through the skin just below the lash line after 1% lidocaine with 1:100,000 epinephrine is injected at the incision site to aid in hemostasis (Fig. 39.1b).
5. A dissection plane is developed with scissors inferior from the incision between the skin and the pretarsal portion of the orbicularis oculi just deep to it. This exposes the pretarsal and then the preseptal portions of the orbicularis oculi muscle (Fig. 39.1c).
6. Between the pretarsal and the preseptal portions of the muscle, a plane is dissected and carried inferiorly deep to the preseptal portion of the orbicularis oculi muscle. This dissection plane is between the preseptal portion of the orbicularis oculi muscle and the orbital septum. This is followed down onto the infraorbital rim (Fig. 39.1d).
7. Once the infraorbital rim is identified, the periosteum over the infraorbital rim can be incised sharply and the fracture can be visualized (Fig. 39.1e).
8. Alternatively, a transconjunctival approach can be performed instead of a subciliary approach (not shown).
9. The periosteum is elevated for a small distance to expose the fracture fragments (Fig. 39.1f).
10. The malar eminence is reduced and rotated into position by lifting the bone with an elevator inserted behind the zygoma from the frontal incision (Fig. 39.1g). The orbital floor is checked for fractures (see Section 40-1).
11. The fractures may be secured with titanium or resorbable minicompression plates, with at least two screws on either side of the fracture line. Resorbable plates require tapping prior to screwing in the plate (Fig. 39.1h).
12. The incisions are closed with 4-0 or 5-0 interrupted Vicryl sutures (Ethicon) in the periosteal layer. The brow skin incision is closed with a 4-0 or 5-0 subcuticular Monocryl (Ethicon). The subciliary skin incision is closed with a 5-0 or 6-0 interrupted or running fast-absorbing gut suture.
13. No dressings or splints are necessary.
Complications
1. Insufficient reduction
2. Wound infection
3. Hardware failure
4. Osteomyelitis
5. Enophthalmos
6. Ectropion/entropion