and Mitrofanis Pavlidis2
(1)
Department of Ophthalmology, Uppsala University Hospital, Uppsala, Sweden
(2)
Augencentrum Köln, Cologne, Germany
9.2.1 Introduction
9.2.2 Surgery
9.2.3 Complications
9.2.4 FAQ
9.3 Macular Holes
9.3.1 Introduction
9.3.2 Surgery
9.3.3 Complications
9.3.4 FAQ
Electronic supplementary material
The online version of this chapter (doi:10.1007/978-3-319-20236-5_9) contains supplementary material, which is available to authorized users.
Electronic supplementary material
for this chapter is accessible online at http://extras.springer.com/ by searching via the ISBN.
9.1 General Introduction
A combined phacoemulsification/vitrectomy is advisable in all patients above 60 years. Ideally the (nonacute) vitrectomy should be performed in a pseudophakic eye, i.e. the cataract surgery should be scheduled before the vitrectomy.
The first difficult surgical step (for a beginner) is the induction of a PVD. In almost all cases of macular holes, a PVD is present. The contrary is the case in macular puckers; a PVD is seldom present.
The next difficult step for a beginner is the peeling itself which is easier in membranes and more difficult for macular holes. The best case for a beginner is a thick macular pucker with uplifted edges. If you feel safe with peeling of puckers, then proceed with macular holes. The appropriate dye for macular puckers is trypan blue, and the appropriate dye for macular holes are Brilliant Blue G. Today, a combined dye with trypan blue and Brilliant Blue G (Membrane Dual®, DORC) is available for staining both an epiretinal membrane and the ILM.
For peeling, only two instruments are required: A good forceps and a retinal scraper (27G retrobulbar cannula, Atkinson, Beaver-Visitec). The retinal scraper elevates an edge in membranes and creates a hole in the ILM in macular hole peeling. Many surgeons use only a forceps. One author (US) uses always a retinal scraper and one author (MP) works only with forceps.
In macular pucker or idiopathic epiretinal membranes (ERM), the epiretinal membrane, which is usually stained with trypan blue, is peeled. Some surgeons recommend a subsequent peeling of the ILM, but there is currently no consensus on this. In a high proportion of cases, the ILM will already be removed together with the ERM. If you wish to peel the ILM after removal of an ERM, then use the dye Membrane Dual® (DORC) from the beginning. It stains the vitreous, the membranes and the ILM.
A gas tamponade is standard for macular holes. There is no standard present for membranes. We perform in most cases an air tamponade to avoid hypotony and inject 0.1 ml triamcinolone if a macular oedema is present. We use triamcinolone without benzalkonium chloride which is possibly toxic for the retina (Vitreal S®, Sooft Italia).
9.2 Epiretinal Membranes
9.2.1 Introduction
Video 9.1: 27G peeling surgery
Video 9.2: 27G macular peeling
The two most important tools for macular peeling are (1) the peeling lens; use a contact lens (e.g. plano-concave contact lens, DORC) or a 60D peeling lens on your BIOM, whichever suits you best, and (2) the peeling forceps. Test different variants of different companies until you find the forceps that suits you best.
9.2.2 Surgery
9.2.2.1 Instruments
1.
27G 3-port trocar
2.
120D lens, for peeling: 60D lens or plano-concave contact lens
3.
Vitreous cutter
4.
Backflush instrument
5.
27G ILM forceps (DORC)
6.
27G retrobulbar cannula (Atkinson)
9.2.2.2 Dye
Membrane: Triamcinolone acetonide, trypan blue
For injection, use a 3 ml syringe with 27-gauge backflush needle (Fig. 9.1).

Fig. 9.1
We refill the dye into a regular 3 cc syringe which is easier to handle than the original syringe
9.2.2.3 Tamponade
Possible air tamponade
Individual Steps
1.
27G 3-port system
2.
Core and peripheral vitrectomy
3.
Staining of the ERM
4.
Peeling of epiretinal membrane
5.
Inspection of periphery
6.
Air tamponade with/without triamcinolone
7.
Removal of the trocars
9.2.2.4 The Surgery Step by Step: Figs. 9.2, 9.3 and 9.4
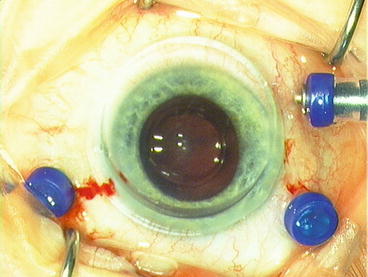
Fig. 9.2
We use depending on the surgeon’s preference a 60D BIOM lens or plano-concave lens (1284.DD, DORC)
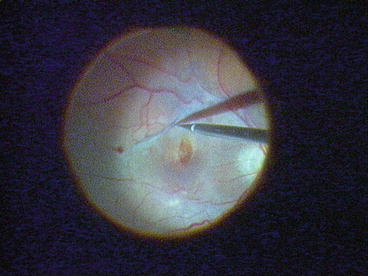
Fig. 9.3
As a retinal scraper, we use a 27G Atkinson cannula
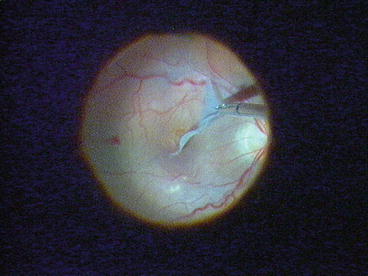
Fig. 9.4
As an intravitreal forceps, we use a 27G endgripping forceps (DORC)
1.
27G 3-port system
2.
Core and peripheral vitrectomy
Insert the trocars. If the patient is older than 60 years, consider a combined phacoemulsification/IOL before the vitrectomy.
Perform a core vitrectomy and induce if necessary a PVD. If you are not sure whether a posterior vitreous detachment is present, stain the vitreous with triamcinolone or trypan blue. If the posterior vitreous detachment has not been successful, you will now recognize the stained premacular vitreous cortex (bursa praemacularis). Continue with a peripheral vitrectomy which has not to be as thorough as in macular holes because no gas tamponade is used.
PVD: If you plan to stain with trypan blue, then use it also for PVD. It makes surgery so much easier. But if you stain the vitreous, you need to restain for the membrane.
3.
Staining of the ERM (epiretinal membrane)
The next step is the staining of the ERM with triamcinolone or trypan blue. Stop the infusion. Then take the syringe with the dye in one hand and eject a few drops of the dye outside the eye in order to avoid blockage of the cannula and injection of air. Then insert the syringe until the tip is placed above the macula and slowly inject a little dye to fall on the macula. After a period of about 15–30 s, turn on the infusion and aspirate the dye with a flute needle or a vitreous cutter.
Surgical Pearls No. 15
Trypan blue: Staining may become difficult if you use the syringe of the company. If too much force is applied during injection, a sudden jet of dye can be injected into the eye which will obscure the view and is cumbersome to remove. We recommend therefore to change the syringes. We use a regular 3 cc syringe instead, which is predictable in its behaviour (Fig. 9.1 ).
Surgical Pearls No. 16
PVD: If you plan to stain with trypan blue, then use it also for PVD instead of triamcinolone. It makes surgery so much easier. But if you stain the vitreous, you need to restain for the membrane.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


