25

Macular Edema Associated with Idiopathic Telangiectasias and Macroaneurysm
Peter Liggett  Nauman Chaudry
Nauman Chaudry
PARAFOVEAL TELANGIECTASIS
“Retinal telangiectasis” is a term first proposed by Reese in 1956 (1) to describe a retinal vascular disorder associated with ectasia and irregular dilation of capillaries in the macula or peripheral retina. Fundoscopic and fluorescein angiographic findings of eyes with loss of macular function associated with retinal telangiectasis have been well described by Gass (2) in 1968. The term “parafoveal telangiectasis” (PT), however, first was used in 1978 by Hutton and colleagues (3), describing the presence of dilated capillaries in the juxtafoveal area. The cause of this condition is unknown; Gass & Oyakama (4) termed this condition “idiopathic juxtafoveal retinal telangiectasis” and divided the disease into several groups based on clinical findings and the purported underlying cause. Gass (2) proposed that in some patients, the telangiectatic capillaries were of congenital or developmental origin (a variant of Coat’s disease), whereas in others, they were an acquired anomaly. Gass and Blodi (5) later modified the original classification system and sub-divided the group into three categories (Table 25-1).
EPIDEMIOLOGY
PT is a relatively rare condition, and precise incidence and prevalence figures have not been established. Patients typically first present in adulthood with decreased vision or scotoma in one or both eyes. Patient characteristics differ for each of these subgroups proposed by Gass and Blodi (Table 25-1). Group 1 patients are usually male and typically have only one eye involved. Patients with group 2 or 3 disease are older and typically have bilateral disease. Both males and females are affected with equal frequency with group 2 disease. Group 3A patients are typically women, whereas group 3B patients are usually men.
A familial tendency may be present in some subtypes (2B, 3A, 3B) (5), and one case of father-to-son transmission of PT has been reported (6).
CONGENITAL PARAFOVEAL TELANGIECTASIS
The common finding on fluorescein angiography in all three groups is the presence of retinal capillary telangiectasis localized to the parafoveal region. Other features are typical (Table 25-1) of a particular group.
Group 1A: Unilateral Congenital Parafoveal Telangiectasis
Group 1A consists typically of men whose mean age at onset of the disease is 40 years. Only one eye is involved in these patients. The telangiectatic vessels are confined to the temporal parafoveal region, and the zone of involvement typically straddles the horizontal raphe (Fig. 25-1A-B). In patients with subtype 1A, the zone of involvement is usually one to two disc diameters in size. The telangiectatic vessels appear as microaneurysmal or saccular dilation of retinal capillaries and are visible biomicroscopically. Retinal capillary leakage is believed to be the principal abnormality in these eyes, and thus exudation is a prominent feature. Lipid exudates are often present at the margin of the zone of telangiectasis. Macular edema and exudation are the major causes of visual loss in these eyes. Visual acuity at presentation usually ranges from 20/25 to 20/40, although 20/200 may occur.
ACQUIRED PARAFOVEAL TELANGIECTASIS
Group 1B: Unilateral Idiopathic Parafoveal Telangiectasis
According to Gass (2), idiopathic PT (IPT) is found in middle-aged men who have more localized disease, with less than two clock hours of telangiectasis. The foveal avascular zone (FAZ) may be significantly smaller in these patients. Mansour and Schachat (7) found that the FAZ was almost completely vascularized in 65% of eyes with IPT studied by fluorescein angiography. The median FAZ in eyes with Group 1 PT was 0.0 mm2 compared with 0.405 mm2 in control eyes. Rarely does this area of telangiectasis have much leakage on fluorescein angiography. Visual acuity is usually better than 20/25.
TABLE 25-1 PARAFOVEAL TELANGIECTASIS CLASSIFICATION (4)
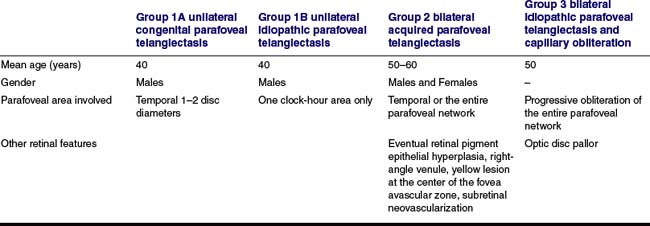
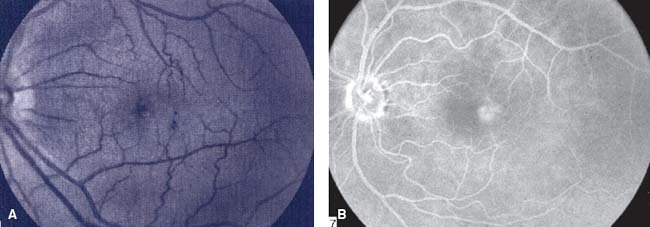
Figure 25-1. Group 1A unilateral congenital parafoveal telangiectasis and macular edema. A: Left eye. B: Late phase fluorescein angiography.
Group 2: Bilateral Acquired Parafoveal Telangiectasis
This is the most common form of IPT. Men and woman are affected equally, and the disease is nearly always bilateral. The telangiectatic capillaries are difficult to see biomicroscopically and often require fluorescein angiography for detection. The telangiectasis always involves the entire parafoveal retina. Multiple refractile, glistening deposits may be seen in the superficial retina overlying the zone of telangiectasis (8). A round yellow spot, 100–300 microns in size, may be present in the foveal center in some eyes.
Gass has described five stages in eyes with Group 2 IPT (5). In the first stage, there is minimal or no evidence of retinal telangiectasis, with only mild staining at the level of the outer parafoveal retina in the late phase of the fluorescein angiography. Stage 3 is characterized by the appearance of dilated venules that extend at right angles from the inner to the outer retina. The right angle venules may appear to drain the outer telangiectatic retinal capillary bed. In stage 4, retinal pigment epithelial hyperplasia develops. The hyperplastic retinal pigment epithelium may form intraretinal pigment plaques and may surround the right angle venules. In stage 5, subretinal neovascularization (SRNV) and fibrosis (Fig. 25-2) develop, typically in the region of intraretinal pigment epithelial migration. SRNV occurs in approximately 14% of eyes with Group 2 IPT. Optical coherence tomography (OCT) has provided further insight into the retinal thickness at the different stages of the natural course of the disease. It appears that, in the presence of retinal staining with fluorescein angiography, there may be no associated retinal thickening. Albani et al. (9) reported the presence of foveal cysts revealed by OCT in stage 3 IPT, but no correlation with fluorescein angiogram was found. Paunescu et al. (10) reported the following OCT features of IPT: a lack of correlation between retinal thickening on OCT and leakage on fluorescein angiography; loss of disruption of the photoreceptor layer; cystlike structures in the fovea and within the internal layers; a unique internal limiting membrane draping across the fovea related to underlying loss of tissue; intraretinal neovascularization near the fovea; and, central intraretinal deposits and plaques.
Gass and Blodi (5) identified a separated subtype of patients, Group 2B, that showed a familial pattern. Group 2B was distinguished from the more common nonfamilial Group 2A by the lack of right-angle venules, superficial retina refractile deposits, and hyperplastic retinal pigment plaques. Acute central visual loss occurs in some patients with the development of neovascularization, which may begin as intraretinal neovascularization. Later follow-up of such cases shows the presence of retinochoroidal anastomosis, which often involves the foveal avascular zone (11).

Figure 25-2. Group 2 bilateral acquired parafoveal telangiectasis. Subretinal neovascularization (SRNV) and fibrosis associated with parafoveal telangiectasis.
Group 3: Occlusive Idiopathic Parafoveal Telangiectasis
The occlusive form is the rarest form of IPT and is characterized by extensive occlusion and loss of parafoveal capillary network, associated with telangiectasis of the remaining parafoveal capillaries. The disease is typically bilateral. Parafoveal fluorescein leakage is virtually absent in these patients. In contrast to Group 1 IPT, in which the FAZ may be small or absent, the FAZ in eyes with Group 3 IPT is enlarged markedly. Despite this marked capillary loss, visual acuity may remain good (20/25 or better in 67%) (5). An atypical case of Group 3 IPT associated with peripheral retinal ischemia and anterior and posterior segment neovascularization has been reported (12).
Gass distinguished patients with subtype 3A from those with subtype 3B, by the presence of an associated central nervous system vasculopathy in patients with 3B. Manifestations of central nervous system disease include optic disc pallor, exaggerated deep tendon reflexes, gait abnormalities, and multiple brain infarcts on magnetic resonance imaging (5).
HISTOPATHOLOGY
Green and colleagues (13) reported on the histopathologic and ultrastructural features of an eye with IPT. The patient was a 58-year-old woman who underwent orbital exenteration for squamous cell carcinoma. Prior to removal of the globe, fluorescein angiography was obtained and revealed bilateral telangiectatic capillaries temporal to the fovea and a clinical picture consistent with Group 2A IPT. On histological examination, however, no telangiectatic capillaries were observed. Rather, there was marked thickening of the capillary wall and narrowing of the lumen. Electron microscopy revealed that the capillary wall thickening resulted from marked proliferation and reduplication of basement membrane in a multilayer arrangement. There was marked degeneration of pericytes and, in some areas, degeneration of endothelial cells. The histopathologic changes observed in this eye are strikingly similar to the retinal vascular abnormalities in patients with diabetes. The patient studied by Green and colleagues had no history of diabetes. Given the lack of true telangiectatic vessels histopathologically, Green and colleagues questioned the use of term “telangiectasis” to describe this condition. They hypothesized that the appearance of telangiectasis of fluorescein angiogram was a result of the diffusion of fluorescein dye through endothelial defects and into the thickened capillary wall.
Gass has suggested that this capillary-wall abnormality was a physical substrate for the “diffusion defect” in patient with group 2 IPT. The histopathology of patients with Group 1 or Group 2 IPT has not been studied.
ASSOCIATION WITH DIABETES MELLITUS
An association between diabetes mellitus and Group 2 IPT has been suggested (13). The histopathologic similarity between the two diseases provides further support for the existence of a relationship. Some investigators have speculated that abnormal glucose metabolism may lead to parafoveal telangiectasis based on findings that 35% of patients with IPT have abnormal glucose tolerance test results (14). Gass and Blodi (5), however, who reported on the largest number of patients, found that only 6.5% of patients with Group 2 IPT developed diabetes. They suggested that diabetes may predispose some patients to develop Group 2 IPT, but that its relative importance is small. Another systemic disease that has been reported to be associated with cases of PT is celiac sprue (15).
A histopathologic study by Eiliassi-Rad and Green (16) showed dilation and proliferation of retinal capillaries into the other retinal and subretinal space. There was a migration of the retinal pigment epithelium within the retina along the telangiectasic vessels. Preretinal neovascularization was also found. Interestingly, there was a sharp demarcation between the edematous and nonedematous retina. With the staining of the retina with fluorescein in eyes with minimal edema, Gas has postulated that it possible that the primary abnormality may be found in the parafoveal retina neural of Muller cells (17).
DIFFERENTIAL DIAGNOSIS
The diagnosis of PT may be made by careful biomicroscopy and fluorescein angiography. PT is a clinical entity that is distinctly different from secondary telangiectasis, which can result from various other diseases. The most common causes of secondary telangiectasis include diabetic retinopathy, venous occlusive disease, radiation retinopathy, hypertensive retinopathy, and ocular ischemic syndrome (5, 18). Most of these secondary causes of telangiectasis tend to produce a diffuse vasculopathy, unlike IPT, which is localized to the parafoveal region (predominantly temporally). Moreover, the presence of associated retinal abnormalities such intraretinal hemorrhage, cotton-wool spots, and retinal neovascularization can help distinguish secondary telangiectasis from IPT.
Venous occlusive disease (particularly small retinal vein occlusions) can produce localized vascular abnormalities, including telangiectasias. The telangiectatic vessels, however, are confined to the distribution of the involved vein, distal to the point of blockage. Thus, the telangiectatic vessels usually do not cross the horizontal raphe. In contrast, in IPT, the telangiectatic vessels typically straddle the horizontal raphe.
Age-related macular degeneration is another entity for which PT may be mistaken. In this disease, the choroidal neovascularization is accompanied by drusen and retinal pigment epithelium (RPE) abnormalities with no evidence of retina capillary disease.
MANAGEMENT
The treatment of macular edema in patients with PT is controversial. There have been no controlled clinical trials. Grid laser photocoagulation to the area of angiographic leakage has been advocated by some investigators (3, 19) who have observed a reduction in macular edema and improvement of visual acuity in treated patients. Others have reported favorable results in a case series in which a number of cases of classic choroidal neovascularization, including PT, received photodynamic therapy (20).
Recently, there has been an increase in the use of intraocular antivascular endothelial growth factor (anti-VEGF). Mandal et al. (21) reported 6 patients treated with intravitreal bevacizumab (Avastin) for subretinal neovascularization secondary to type 2A idiopathic juxtafoveal telangiectasia. After a follow-up of 4.2 months, the visual acuity improved two or three lines as did the mean central foveal thickness. This is a small series and longer follow-up is required. Moon et al. (22) reported one case with complete resolution of macular edema after intravitreal bevacizumab injection in short term follow-up. Intravitreal triamcinolone injection is been also reported for the treatment of macular edema secondary to idiopathic juxtafoveal telangiectasis in one patient (23).
RETINAL ARTERY MACROANEURYSMS
Retinal arterial macroaneurysms are an acquired retinal vascular abnormality. These isolated dilations of the major retinal arterial branches are found within the posterior pole and are associated with systemic hypertension, arteriosclerosis, retinal emboli and cardiovascular disease. Robertson, in 1973 (24), coined the term “macroaneurysm” for a retinal arterial lesion with the following characteristics: saccular or fusiform arterial swelling, located within the first three orders of the retinal arteriole tree, and usually situated at the arterial bifurcation. Most commonly, retinal macroaneurysm affects patients in the sixth and seventh decades of life. Numerous studies have found 70% to 80% of the patients to be women. A large collaborative series by Schatz et al. described the findings in 130 eyes of 120 patients; they found two-thirds of these patients to be hypertensive (25, 26). It presents unilaterally in more than 90% of patients.
CLINICAL SYMPTOMS AND FINDINGS
The majority of patients are asymptomatic if the macula is not involved, but the most common clinical symptom is acute decrease in central visual acuity due to retinal edema, exudation, or hemorrhage (27). Patients may have also other visual changes such as shadows of “floaters.”
Macroaneurysms typically present as round or fusiform dilation of the retinal arteriole that may be several times the caliber of the arteriole (Fig. 25-3A). Variable degrees of arterial wall hyalinization and surrounding intraretinal lipid and hemorrhage are frequently present. They occur mostly in the superotemporal retinal vasculature (52%), followed by inferotemporal (38%), inferotemporal (5%), and superonasal vessels (5%) (28). If pulsatile macroaneurysm is present, some investigators speculate that a greater risk of vitreous hemorrhage exists (29). Schatz et al. (26) coined the term hourglass hemorrhage to describe the simultaneous presence of both a subretinal and preretinal hemorrhage secondary to the macroaneurysm. Secondary vitreous hemorrhage occurs in approximately 10% of eyes but is rarely recurrent. Hemorrhage in the space beneath the retinal pigment epithelium may produce a dark lesion simulating an ocular melanoma (30) or a lesion associated with age-related macular degeneration. Table 25-2 shows the most common retinal disorders to be considered in the differential diagnosis of retinal artery macroaneurysms.
ANGIOGRAPHIC FEATURES
Fluorescein angiography in an eye with retinal macroaneurysm may disclose early uniform filling (Fig. 25-3B). The hemorrhage may also partially or completely obscure the aneurysm. In those cases, indocyanine green angiography could be helpful in establishing the diagnosis and influencing the management of these patients who present with submacular or premacular hemorrhage (31). The appearance of the late phase of the fluorescein angiography varies, ranging from little staining of the vessel wall to marked leakage. The lipid often present in the macular area fails to block fluorescein unless the amount of exudation is massive.
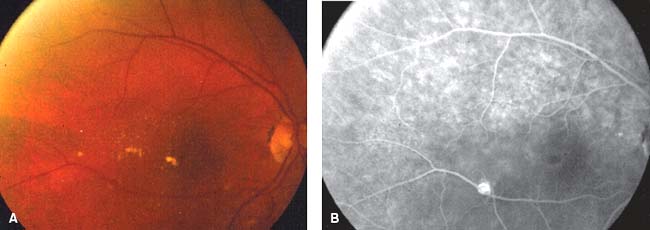
Figure 25-3. A: Retinal arterial macroaneurysm with surrounding lipid exudate. B: Early phase fluorescein angiography showing complete filling of retinal artery macroaneurysm.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


