(1)
Alo Eye Care, Kolkata, India
Keywords
Lid reconstructionLid margin defectsLateral CanthotomyPunctumTenzel rotational flapMcGregor Z plastyCheek flapHughes procedureSkin flapsPosterior lamellar graftsMustarde’s cheek rotational flap13.1 Small Central Eyelid Margin Defects (Direct Closure)
13.1.1 Indications
Defects involving ≤30 % of the lower eyelid in young patients or ≤45 % in elderly patients
Cases in which the two cut edges can be brought together without undue tension
13.1.2 Technique
Be sure that all margins are tumor-free.
If the excised tissue defect does not extend beyond the inferior edge of the tarsal plate, the cuts are extended to cross the inferior margin of the tarsal plate.
An inverted triangle is cut inferior to the defect. The base of the triangle should start below the inferior extent of the tarsal plate (to prevent notching and irregular contouring of the newly formed lid margin).
The wound should look like an inverted pentagon.
The orbicularis muscle is separated from the tarsal plate at the edges to allow better placement of sutures.
The lid defect is repaired in two layers, as described in Chap. 11.
13.1.3 Other Variations/Options
Bringing the cut edges together with tooth forceps will provide a good estimate of the feasibility of this approach.
If undue tension on the suture line is anticipated, a lateral canthotomy should be planned. Details of this procedure are discussed in the next section.
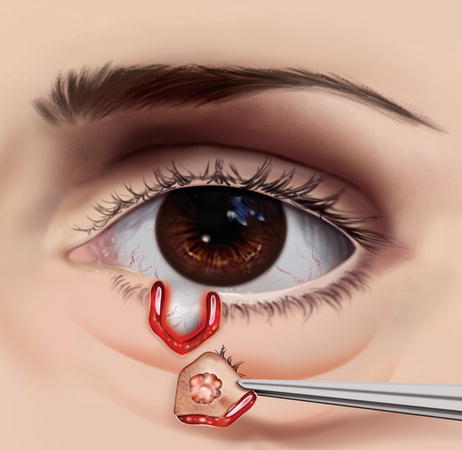
Fig. 13.1
Direct closure. A central full-thickness inverted-pentagon marginal tumor has been excised

Fig. 13.2
Direct closure. Interrupted sutures are applied through the gray line and tarsus

Fig. 13.3
Direct closure. More interrupted sutures are applied
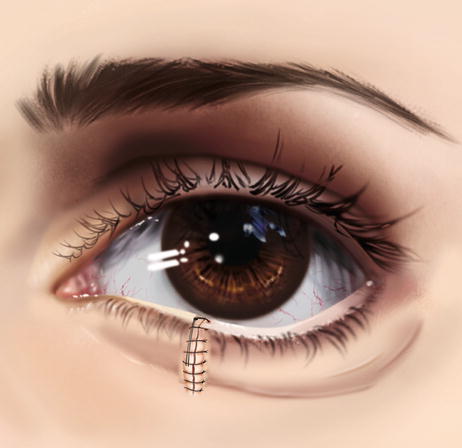
Fig. 13.4
Direct closure. Skin suturing is complete

Fig. 13.5
Direct closure. Full-thickness eyelid defect

Fig. 13.6
Direct closure. Three interrupted sutures through the deeper layers of the cut ends

Fig. 13.7
Direct closure. Gray line suture

Fig. 13.8
Direct closure. Two weeks after direct lid closure
13.2 Small to Medium Central Eyelid Margin Defects That Cannot Be Closed by Direct Apposition (Lateral Canthotomy)
13.2.1 Indications
Similar to those of direct closure but including cases in which there seems to be undue stress on the apposition line.
13.2.2 Technique
If undue tension on the suture line is anticipated, a lateral canthotomy should be planned.
An artery forceps is applied over the lateral canthus horizontally.
The clamp is crushed so that on removal, the serrated indentations of the arterial forceps are visible over the lateral canthus.
Westcott scissors then are applied through the crushed tissue (curved slightly downward to cut the lower canthal ligament). Cutting of the lateral canthal ligament can usually be felt as a sensation of something giving way. This may be confirmed by a sudden increase in mobility of the lower lid.
A skin incision is made over the lateral canthus, angled slightly superior in case a rotational flap is necessary.
Reapproximation of the defect is attempted with a pair of skin hooks; they now should be apposed easily.
The lid defect is sutured in two layers, as discussed earlier.
A few interrupted sutures may be applied between the conjunctiva and the skin at the lateral canthus. This will give a good contour to the lateral angle.
13.2.3 Other Variations/Options
The lateral canthus may be left to granulate by itself.
If undue tension remains on the lid margin, the skin must be mobilized from the superio-lateral aspect of the orbit by a Tenzel rotational flap.

Fig. 13.9
Lateral canthotomy. Lower lid defect that cannot be closed by direct closure
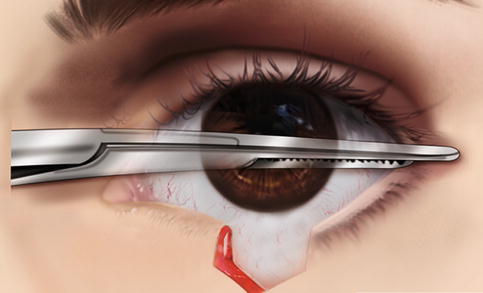
Fig. 13.10
Lateral canthotomy. The lateral canthus is crushed with artery forceps
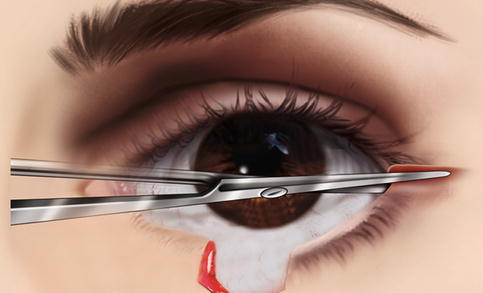
Fig. 13.11
Lateral canthotomy. The lateral canthal ligament is cut
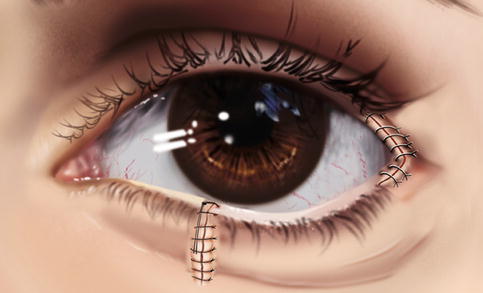
Fig. 13.12
Lateral canthotomy. Interrupted sutures are applied to form a V at the canthal angle, and the mobilized cut ends are approximated and closed as in direct closure
13.3 Small Lateral or Medial Eyelid Margin Defects
13.3.1 Indications
Small lower lid full-thickness defects near the medial or lateral canthus in which tarsus is present only on one side or edge.
13.3.2 Technique
Because the tarsal plate is absent on one edge of the repair, special care must be taken in approximating the tissue.
Here, the defect also is repaired in two layers, but with a slight variation.
The deeper layer suture is passed, as is done through the tarsus, from one side to come out through the cut end.
As there is no tarsal plate on the other side, the suture is passed through the deeper soft tissue, with care taken not to come out through the skin or to injure the canaliculi. A surgical knot is applied.
If the medial canthal ligament can be located, the soft tissue bite is passed through it.
One or two similar sutures are applied above or below the first knot.
Once the skin is in proximity, the lid skin is repaired with three to five interrupted 6/0 Vicryl or Nylon sutures.
13.3.3 Variations/Options
Care must be taken to approximate the lid margin properly, as the lid with tarsus is thicker than the area of canthus in which it is being sutured.
Lesions in the area of the medial aspect of the lower lid may lie over the canaliculi, or may involve them.

Fig. 13.13
Lower lid full-thickness defect near the lateral canthus

Fig. 13.14
Full-thickness defect near the lateral canthus. Approximation and repair are done in two layers
13.4 Defects Extending Medial to the Punctum
13.4.1 Indications
Any lower lid full-thickness defect encroaching on the medial canthus in which the lower punctum, along with a section of canaliculi, has been sacrificed.
13.4.2 Technique
Basic repair is similar to what is done to repair medial marginal defects, as discussed in detail earlier. The challenge is in repairing the lacrimal drainage system and keeping it patent.
If the cut end of the canaliculus can be located clearly, it may simply be snipped and marsupialized with the surrounding conjunctiva, which works quite well.
In difficult cases and in younger patients, an attempt may be made to locate the cut end of the canaliculus and to insert a lacrimal tube into the sac. The free-cut outside end of the tube is kept long and fixed to the surrounding skin so it is not displaced. The tube is removed after 6–8 weeks.
Another option is to pass a lacrimal tube through the cut end of the lower canaliculus, as well as through the upper canaliculus; guide it through the nasolacrimal duct (NLD) into the nose; tie a knot; and keep the bicanalicular tube in place for 3 months. After 3 months, with nasal endoscopic guidance, the tube is cut over the medial canthus and pulled through the nose.
13.4.3 Other Variations/Options
Another option is the Mini-Monoka monocanalicular stent, which remains in position because of its design and prevents tube migration.
If most of the canaliculus has been excised, reconstruction of the tear drainage system is planned as a second step after the patient is evaluated (because epiphora rarely occurs in patients older than 60 years or those in whom the upper canaliculus is still patent).
Another option is conjunctival dacryocystorhinostomy performed as a later, repeat procedure.
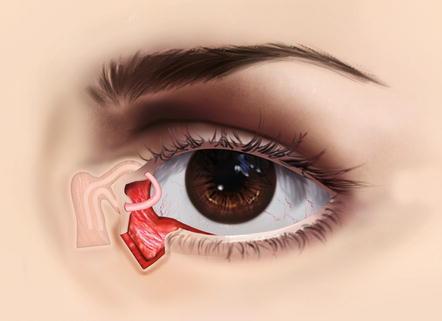
Fig. 13.15
Lower lid defects extending medial to the punctum. Bicanalicular intubation has been done

Fig. 13.16
Lower lid defects extending medial to the punctum. As elsewhere, the repair is carried out in two layers

Fig. 13.17
Lower lid defects extending medial to the punctum. Post repair, with the tube in position

Fig. 13.18
Lower lid defects extending medial to the punctum. An alternative is monocanalicular intubation, with the medial end of the tube kept coiled in the sac. The cut lateral end is fixed to the surrounding lid skin to prevent migration

Fig. 13.19
Lower lid defects extending medial to the punctum. Another option is the Mini-Monoka monocanalicular stent, which remains in position because of its design and prevents tube migration
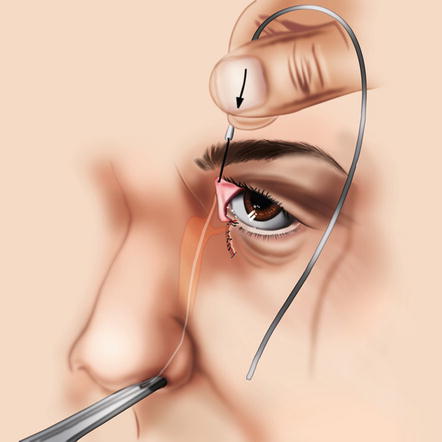
Fig. 13.20
Lacrimal tube insertion through the NLD. A lacrimal tube has been passed through the upper canaliculus and guided into the NLD
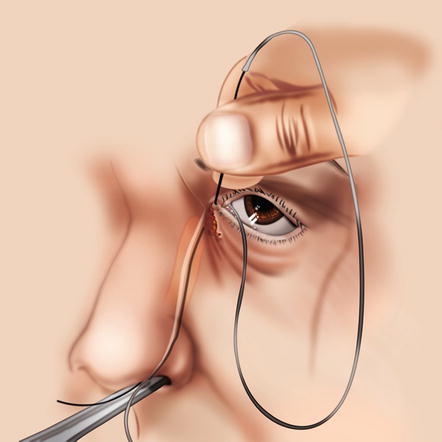
Fig. 13.21
Lacrimal tube insertion through the NLD. The other end of the tube is guided through the cut end of the lower canaliculus, through the NLD, and into the nose

Fig. 13.22
Lacrimal tube insertion through the NLD. A knot is tied, and the bicanalicular tube is kept in place for 3 months
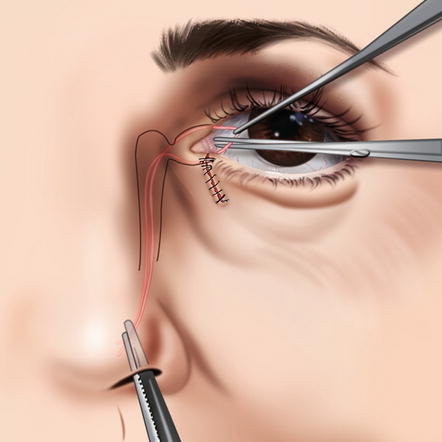
Fig. 13.23
Lacrimal tube insertion through the NLD. After 3 months, with nasal endoscopic guidance, the tube over the medial canthus is cut and pulled through the nose

Fig. 13.24
Marsupialization of the inferior canaliculus. A probe is passed through the lower canaliculus to keep track of its position

Fig. 13.25
Marsupialization of the inferior canaliculus. The requisite area of canaliculus has been excised

Fig. 13.26
Marsupialization of the inferior canaliculus. The cut end of the canaliculus is reconfirmed and sutured to the surrounding conjunctiva

Fig. 13.27
Marsupialization of the inferior canaliculus. Six weeks after surgery, healing is satisfactory

Fig. 13.28
Marsupialization of the inferior canaliculus. A close-up view of the canaliculus shows it is slit-like and performing perfectly
13.5 Medium to Large Lower Eyelid Defect (Tenzel Rotational Flap)
13.5.1 Indications
Full-thickness lid margin defects in which the lid cannot be apposed despite lateral canthotomy
Defects involving 50–60 % of the lower lid, situated in the central portion, where a cut end of the tarsal plate is available on both side
13.5.2 Technique
A semicircular skin incision is marked from the lateral angle. The incision line is arched upward to cross the superior lateral periorbital skin. Superiorly, it should not extend beyond the level of the lateral aspect of the eyebrow, and it should not cross the skin in front of the tragus.
Lateral cantholysis is performed as described earlier.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


