Purpose
To evaluate long-term visual outcome and investigate the prognostic factors after anti–vascular endothelial growth factor (VEGF) therapy for polypoidal choroidal vasculopathy (PCV).
Design
Retrospective study.
Methods
Analyses were done among 36 eyes (36 patients) with naïve PCV that were treated with intravitreal ranibizumab injections and completed at least 3-year follow-up. All clinical data, including baseline characteristics; imaging data from fluorescein angiography, indocyanine green angiography, and optical coherence tomography; presence of recurrence; and best-corrected visual acuity (BCVA) were investigated.
Results
During mean follow-up of 42.58 ± 12.59 months, mean numbers of anti-VEGF injection were 11.45 ± 7.81. Twenty-four eyes (66.7%) showed at least 1 recurrence during follow-up. Mean baseline BCVA was 0.68 ± 0.43 logMAR (20/95 Snellen equivalent), and 0.78 ± 0.53 logMAR (20/120 Snellen equivalent) at 36 months ( P = .307). Mean BCVA was significantly improved at 1 month ( P = .018), and improvement was maintained until 12 months ( P = .044), then deteriorated. Among baseline characteristics, greatest lesion diameter (B = 0.219, P = .001) and pigment epithelial detachment (B = 0.362, P = .025) were significantly correlated with long-term visual outcome. Recurrence during follow-up (B = 0.371, P = .024) was also significantly correlated with long-term visual outcome.
Conclusion
Significant visual improvement by anti-VEGF therapy was maintained during the first year of initial treatment; however, vision then deteriorated during long-term follow-up. Smaller lesion size, absence of pigment epithelial detachment at baseline, and no recurrence during follow-up were significantly correlated with better long-term visual outcome.
Polypoidal choroidal vasculopathy (PCV) has been increasingly recognized as a major cause of vision loss throughout the world since its introduction as a new clinical entity in 1990. PCV is characterized by orange-red protrusions on funduscopy and polyp-like pooling of dye on indocyanine green angiography (ICGA). Abnormal branching vascular networks and pigment epithelium detachment are frequently associated with the polypoidal lesions. PCV accounts for up to 50% of presumed exudative age-related macular degeneration (AMD) in Asian populations.
Although the exact pathogenesis of PCV is still under investigation, photodynamic therapy (PDT) and anti–vascular endothelial growth factor (VEGF) therapy are currently used for treating PCV. Using anti-VEGF therapy is advocated by several studies. Anterior chamber fluid contains increased VEGF levels in PCV patients. Histologic studies revealed strong VEGF expression in choroidal vascular endothelial cells and retinal pigment epithelium (RPE) cells in PCV patients. These findings suggest that VEGF plays a role in PCV pathogenesis and support using anti-VEGF agents, such as ranibizumab, to treat PCV. Complications of PDT are another reason to preferentially administer anti-VEGF therapy to treat PCV. In addition to hemorrhagic tendency of PCV itself, PDT can cause further hemorrhagic complications in these patients. Complications such as massive subretinal hemorrhage and vitreous hemorrhage occur in up to 30% of PCV patients after PDT and may lead to significant visual deterioration.
Anti-VEGF therapy for PCV showed favorable visual outcomes during 6- to 12-month follow-ups in several studies. However, anti-VEGF therapy seems to have limited efficacy in polypoidal lesion regression. A recent angiographic study reported that complete disappearance of polypoidal lesions was achieved in only 26% of PCV eyes after 3 monthly injections of ranibizumab, although exudative changes regressed with concomitant improvement of visual acuity. Long-term validations of anti-VEGF therapy for PCV remain limited, whereas long-term favorable visual outcome has been validated with PDT for PCV.
Additionally, little is known about the prognostic factors for PCV. One study identified baseline lesion size, age at diagnosis, and baseline BCVA as predictive factors of visual acuity 1 year after PDT for PCV. However, studies concerning visual prognostic factors after anti-VEGF therapy are limited in number and showed inconsistent results. One report compared factors associated with the response of typical AMD and PCV to intravitreal ranibizumab therapy. They reported that age and baseline lesion size were significantly associated with visual prognosis in typical AMD but not in PCV. However, another study revealed that larger PCV lesion size is associated with poor visual outcome after anti-VEGF therapy.
In the present study, we evaluated long-term treatment efficacies and visual outcomes at least 3 years after anti-VEGF monotherapy with intraocular ranibizumab injections for PCV. We also investigated prognostic factors for long-term visual outcomes in these patients.
Methods
Enrollment of Study Subjects
We retrospectively reviewed 36 eyes of 36 patients with treatment-naïve PCV who fulfilled the inclusion and exclusion criteria. The patients were treated at the Vitreoretinal Service Clinic of Yonsei University Medical Center between January 2009 and December 2012. All patients underwent intravitreal ranibizumab injections for PCV and completed at least 3 years of follow-up after the first treatment. Written informed consent was obtained from all participants at the time of treatments. Those included in this study were declined any PDT at initial treatment and retreatment because of possible hemorrhagic complications of PDT itself after full explanation of treatment options for PCV. This retrospective study was approved by the Institutional Review Board of Yonsei University College of Medicine and was conducted in accordance with the tenets of the Declaration of Helsinki. Inclusion criteria were: (1) symptomatic macular PCV with subfoveal leakage on fluorescein angiography (FA); (2) presence of branching vascular networks and polypoidal lesions on ICGA; and (3) follow-up at least 36 months after initial treatment. Exclusion criteria were: (1) any treatment for PCV including laser photocoagulation, transpupillary thermotherapy, radiotherapy, and PDT (2) other concomitant ocular diseases, such as diabetic retinopathy, high myopia, vein or artery occlusion, and epiretinal membrane; and (3) any systemic contraindications to angiographic dyes. PCV diagnosis was based on ICGA findings of the abnormal branching vascular networks and polypoidal lesions.
Examinations
All patients received a complete ocular examination, including best-corrected visual acuity (BCVA) testing using a decimal visual acuity chart, slit-lamp biomicroscopy, dilated fundus examination with indirect ophthalmoscopy, color fundus photography, digital FA, ICGA, and optical coherence tomography (OCT) (Spectralis; Heidelberg Engineering, Heidelberg, Germany) at baseline. FA and ICGA were obtained using the Heidelberg Retina Angiograph system (HRA-2; Heidelberg Engineering) with a confocal scanning laser ophthalmoscope.
Choroidal neovascularization (CNV) type was determined by FA. Greatest linear dimension (GLD) and area of the lesion were determined by the ICGA. Polypoidal lesions were classified according to angiographic characteristics. The locations of PCV lesions were subdivided into 3 categories: subfoveal, juxtafoveal, and extrafoveal. In addition, formations of the PCV lesions were classified into 3 categories: single, cluster, and string. In addition, PCV were classified into 2 categories by the number of discrete areas of polypoidal lesions: single and multiple. Greatest linear dimension included the entire branching vascular network vessels and polypoidal lesions at the early phase of ICGA, assessed using HRA-2 software. The PCV lesion area was also measured manually with the HRA-2 software. When measuring the greatest linear dimension and the PCV lesion area, pigment epithelial detachment (PED) was not counted if there was no underlying vascular component.
Baseline OCT characteristics were also investigated, including intraretinal fluid cyst, subretinal fluid (SRF), and PED at the fovea. Central retinal thickness (CRT) was defined as the distance between the internal limiting membrane and the inner surface of the RPE and was measured manually at the fovea. The SRF and intraretinal fluid cyst were included in the CRT measurements, whereas PED was not.
Intravitreal Ranibizumab Injection
Intravitreal ranibizumab injections (0.05 mg Lucentis; Genentech, South San Francisco, California, USA) were administered in the operating room under strict aseptic conditions. Ranibizumab was injected into the vitreous cavity through the superior sclera using a 30-gauge needle, at a position 3.5 mm posterior to the corneal limbus in phakic eyes and 3.0 mm posterior in aphakic/pseudophakic eyes. Pressure was applied to the injection site using a sterile cotton swab for 1 minute to prevent leakage. After injections, patients were instructed to apply antibiotic eye drops for 1 week.
Follow-up and Reinjection Protocols
Follow-up visits were arranged 1 week after each baseline treatment and then 1, 3, 6, 12, 24, and 36 months afterward, with examination including BCVA, dilated fundus examination with indirect ophthalmoscopy, and OCT. After 3 monthly injections of ranibizumab, FA and ICGA were additionally performed to evaluate treatment outcome. Patients were asked to return to the clinic immediately in cases of visual loss and/or metamorphopsia recurrence. Additional FA, ICGA, OCT, and dilated fundus examinations were performed whenever physicians suspected PCV recurrence or visual loss and/or metamorphopsia recurrence. We defined PCV recurrence as the reappearance of active PCV lesions on ICGA with subfoveal leakage on FA after at least 6 months without treatment. Earlier detection of active PCV with leakage before 6 months was considered to be persistence of the original lesion, rather than recurrence.
Retreatment was considered if any of the following changes were observed during follow-up: (1) any visual acuity loss determined with a decimal visual acuity chart with OCT evidence of fluid in the macula; (2) an increase in OCT CRT of at least 100 μm; (3) new macular hemorrhage; or (4) evidence of persistent fluid on OCT 1 month after the previous injection. When reinjection was required, ranibizumab was intravitreally injected within 1 week.
Statistical Analyses
Patient characteristics were retrieved from their medical charts, including age at initial diagnosis, sex, and BCVA as determined using Snellen charts. Snellen BCVA results were converted to a logarithm of the minimal angle of resolution (logMAR) value for statistical analysis. After BCVA was converted to logMAR, we classified the patients into 3 groups: improved, stable, and deteriorated BCVA. An improvement of ≥0.3 in logMAR visual acuity was defined as improved VA, and a decrease of ≥0.3 logMAR visual acuity was defined as deteriorated. All examination data at baseline and at 1-, 3-, 6-, 12-, 24-, and 36-month follow-ups were interpreted retrospectively.
IBM SPSS 18.0 software for Windows (SPSS/IBM Corporation, Chicago, Illinois, USA) was used for statistical analyses. To compare the mean BCVA at each time point and baseline BCVA, a paired t test was used. The 2-sample t test was used for analysis of continuous variables, and the χ 2 test was used for categorical variables. Stepwise logistic regression was used for determining predictive factors for long-term visual prognosis after anti-VEGF therapy for PCV. Mauchly’s test of sphericity and Kolmogorov-Smirnov analysis were used to confirm statistical validity. Differences with P < .05 were considered statistically significant.
Results
Baseline Characteristics
In total, 36 eyes of 36 patients who had completed at least 3 years of follow-up visits after the initial anti-VEGF therapy were analyzed. Patients had a mean age of 68.42 ± 7.93 years and showed a male predominance (24 male patients, 75%). Patient clinical details are listed in the Table . Baseline FA showed occult CNV in all eyes. Baseline ICGA showed a dilated network of inner choroidal vessels with terminal hyperfluorescent polypoidal lesions in all cases.
| Characteristics | |
|---|---|
| Age of onset (y) | 68.42 ± 7.93 a |
| Male/female, n (%) | 24 (75%)/12 (25%) |
| Greatest linear dimension (mm) | 2.30 ± 1.21 a |
| Central retinal thickness (μm) | 368.38 ± 106.54 a |
| Lesion area (μm 2 ) | 3805.71 ± 2111.10 a |
| Lesion location | |
| Subfoveal | 17 (47%) |
| Juxtafoveal | 11 (31%) |
| Extrafoveal | 8 (22%) |
| Baseline OCT characteristics | |
| Subretinal fluid | 35 (97%) |
| Intraretinal cyst | 11 (31%) |
| Pigment epithelial detachment | 15 (42%) |
| Polyp formation | |
| Single | 19 (52.8%) |
| Cluster | 14 (38.9%) |
| String | 3 (8.3%) |
| Discrete polyp area | |
| Single | 35 (97.2%) |
| Multiple | 1 (2.8%) |
| BCVA at baseline | |
| logMAR | 0.68 ± 0.43 a |
| (Snellen equivalent) | (20/95) |
Visual Outcomes After Intravitreal Ranibizumab Monotherapy for Polypoidal Choroidal Vasculopathy
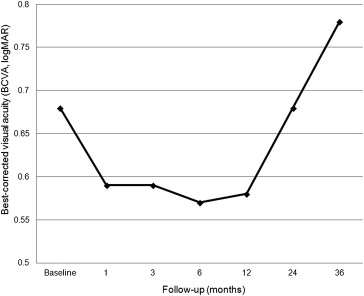
The mean BCVA was 0.68 ± 0.43 logMAR (20/95 Snellen equivalent) at baseline and 0.78 ± 0.53 logMAR (20/120 Snellen equivalent) at the 36-month follow-up. Changes of mean BCVA from baseline during the follow-up periods are shown in Figure 1 . Compared with baseline BCVA, the mean BCVA improved 1 month after initial treatment ( P = .018), and significant visual improvement continued until 12 months ( P = .044). However, after 24 months, the mean BCVA returned to a level that was not significantly different from baseline BCVA ( P = .913), and this was maintained through 36 months of follow-up ( P = .307).
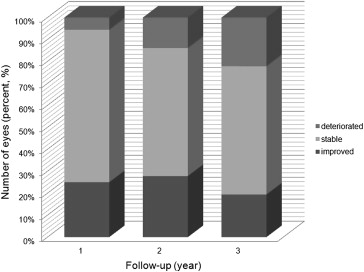
After assessing BCVA at each follow-up visit, we categorized the patients into 3 groups, based on their BCVA change from baseline: improved, stable, and deteriorated visual acuity. The mean BCVA improved in 9 eyes (25.0%), stabilized in 25 eyes (69.4%), and deteriorated in 2 eyes (5.6%) at 1 year. In the deteriorated group, 1 eye had active polypoidal lesions with exudative fluid, and the other eye had subretinal scarring with adjacent RPE atrophy. After 3 years, 7 eyes (19.4%) showed improved vision, 21 eyes (58.4%) were stable, and 8 eyes (22.2%) had deteriorated ( Figure 2 ). Among the 8 eyes with deteriorated vision at 3 years, 2 eyes had active polypoidal lesions with exudative fluid, 2 eyes had subretinal fibrosis, 1 eye had RPE atrophy, and 3 eyes had subretinal fibrosis with RPE atrophy.
Intravitreal Ranibizumab Injections During Follow-up
During a mean follow-up of 42.58 ± 6.59 months, patients received an average of 11.45 ± 7.81 ranibizumab injections. Two eyes showed persistent leakage on angiography and subretinal fluid on OCT during follow-up. Except for these 2 eyes with persistent leakage, the other eyes received an average of 4.81 ± 0.50 intravitreal ranibizumab injections to achieve first remission. During the first year of treatment, mean 5.39 ± 0.50 injections were performed per patient. Mean 3.00 ± 0.53 injections and 3.72 ± 1.01 injections were administered during the second and third years, respectively.
Changes in Lesions After First Treatment
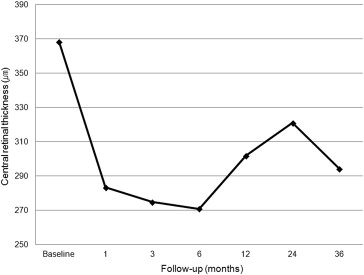
We investigated lesion changes before and after anti-VEGF therapy for PCV by FA, ICGA, and OCT. The mean CRT decreased from 368.34 ± 106.54 μm at baseline to 294.20 ± 114.85 μm at 3 years ( P = .045). The changes of mean CRT at each time point are shown in Figure 3 . We evaluated polyp regression rates determined by ICGA at 3 months after initial treatment. Eight eyes (22.2%) showed polyp regression at 3 months, and 11 eyes (30.6%) had at least 1 complete polyp regression at any time point during follow-up. No complete regression of abnormal branching vascular networks was observed.
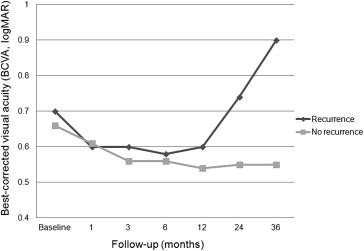
Recurrence of Polypoidal Choroidal Vasculopathy
Recurrences of PCV were noted in 24 out of 36 eyes (66.7%). The mean recurrence interval was 15.92 ± 8.93 months, and mean number of recurrences was 1.70 ± 0.20 times during follow-up. The average number of anti-VEGF injections was 11.29 ± 7.34 in the eyes with recurrent PCV vs 4.91 ± 1.49 injections in eyes without recurrence ( P = .019). The eyes with recurrence showed similar BCVA until 24 months when compared with eyes without recurrence ( P = .800 at baseline, P = .933 at 1 month, P = .745 at 3 months, P = .918 at 6 months, P = .694 at 12 months, and P = .104 at 24 months). After 36 months, however, eyes with at least 1 recurrence showed significantly worse mean BCVA than eyes without recurrence ( P = .049). The changes of mean BCVA in the anti-VEGF-treated group are shown in Figure 4 .