Purpose
To analyze the characteristics and long-term outcomes of patients that underwent pediatric penetrating keratoplasty (PPK) for herpes simplex virus (HSV) keratitis.
Design
Retrospective, interventional, consecutive case series.
Methods
Observational report of outcomes and findings for 9 patients with history of HSV keratitis that underwent PPK and were followed in a single institution. Difference between the median preoperative and final best-corrected visual acuity (BCVA) was assessed and the outcomes are reported.
Results
We included 9 eyes; median age at the moment of the PPK was 14 years. The median initial BCVA was 20/400 (range 20/60 to hand motion) and final was 20/50 (range 20/30 to 20/400) ( P < .05). Follow-up was a median of 94 months. Complications in these patients included glaucoma (1), graft rejection (1), recurrence of disease (1), and amblyopia (3). No graft failures were present.
Conclusion
The long-term outcomes with PPK for HSV keratitis in children provide improvement in BCVA when not compromised by amblyopia.
Pediatric penetrating keratoplasty (PPK) represents a challenge in both surgical technique and postoperative management. The eye of the pediatric patient is smaller, the sclera and cornea are less rigid, and there is increased positive posterior vitreous pressure, with a stronger inflammatory reaction. Follow-up is sometimes difficult owing to poor patient cooperation and the inability of young children to communicate postoperative symptoms. Nevertheless, corneal transplantation is often needed to improve visual acuity, preserve ocular integrity, and avoid amblyopia.
Herpes simplex virus (HSV) keratitis in children warrants further research. Previous reports have addressed the clinical characteristics, complications, and recurrence rate of HSV keratitis in children; however, literature regarding the long-term outcomes of corneal transplantation in these patients is scarce.
The aim of this study is to analyze the characteristics of children that underwent PPK for HSV keratitis and to report their long-term outcomes.
Methods
A hospital-based noncomparative, retrospective, interventional clinical case series was performed. The study was approved by the Institutional Review Board and the ethics committee, and was performed in accordance with the tenets of the Declaration of Helsinki. Children aged 17 years or younger diagnosed with HSV keratitis that were treated with penetrating keratoplasty at the Instituto de Oftalmologia Conde de Valenciana in Mexico City were included, and their electronic medical records were reviewed. When available, patients were contacted and reevaluated.
Patients were diagnosed by their clinical history and slit-lamp examination based on characteristic herpetic keratitis that responded well to the treatment of antivirals and corticosteroids, and sometimes confirmed by either viral culture or polymerase chain reaction. Patients with atypical manifestations, confusing clinical presentation, and no laboratory confirmation were excluded from this study.
Preoperatively, patients were examined and uncorrected distance visual acuity and best-corrected visual acuity (BCVA) recorded. When pertinent, contact lens over-refraction was performed. A complete ophthalmic examination, including biomicroscopic examination of the anterior segment, intraocular pressure, and, when possible, funduscopy, was performed. Corneal sensitivity was tested in all patients, and when cooperation was feasible a Cochet-Bonnet esthesiometer was used; however, in most cases a thread of a cotton swab was employed for that purpose and results were compared with the other eye.
Demographics including sex, age at presentation, and age at time of surgery were registered. The clinical presentation was recorded as epithelial keratitis, stromal keratitis (either immune mediated or necrotizing), and endotheliitis (linear, disciform, or diffuse) or a combination of the above. When available, the number of recurrences was also recorded. History of systemic disease was investigated, specifically atopic skin disease, asthma, and other allergies; disease status was classified as active either if inflammation at the cornea was present or if perforation was present or imminent, and inactive if a corneal scar was present in the absence of inflammation. Visual acuity was measured with Allen picture figures, LEA symbols test, HOTV, illiterate E, or Snellen visual charts depending on age. BCVA before PPK and at the final follow-up was measured with rigid contact lens over-refraction; time of prophylactic acyclovir and complications are reported.
Prophylactic oral acyclovir was indicated for at least 6 months before surgery and continued postoperatively indefinitely: a dose of 400 mg/d in those older than 2 years, divided in 2 doses, and 400 mg 2 times daily when the patients were able to take pills. Tolerance to medication was recorded, and for patients with long-term prophylaxis, kidney and liver functions tests were routinely ordered biannually.
All patients were treated with a PPK performed at our institute, based on rehabilitation for optical purposes. Surgeries were performed under general anesthesia, with the use of a Flieringa ring and donor grafts oversized by 0.5-1.0 mm. Sixteen 10-0 nylon interrupted sutures were used in all patients. At the end of the surgery, all patients were given topical steroids and antibiotics. Postoperatively, topical prednisolone acetate 1% was administered 4-6 times a day initially and then in tapering doses, with topical antibiotic drops for 1 month. Occlusion therapy was undertaken in patients suspected to have amblyopia. Suture removal was performed in all cases at the slit lamp owing to patient cooperation, and it was completed in most cases by 1 year.
Ocular hypertension was defined as intraocular pressure greater than 21 mm Hg as measured with applanation tonometer in 2 different measurements, or if patients had antihypertensive drops. Glaucoma was defined as ocular hypertension and increased cup-to-disc ratio and abnormal optic nerve, optical coherence tomography, or automatized visual fields. Graft rejection was considered by the biomicroscopic appearance of an anterior chamber reaction with keratic precipitates exclusively on the donor endothelium, by an endothelial or epithelial rejection line, or by graft edema with associated new keratic precipitates. Herpetic recurrences were considered as keratitis with edema confined to the endothelial precipitates adhering to both the donor and host endothelium, and iritis. In both cases, patients were treated with systemic acyclovir and topical corticosteroids. Graft failure was defined as corneal edema in the absence of inflammation that did not respond to steroids.
Statistical Analysis
Categorical variables were evaluated by descriptive statistics using percentages; for continuous variables, median and range were used. The difference between the median preoperative BCVA and final BCVA was assessed through paired t test, and the comparison between younger (12 and younger) and older (13 and older) patients was performed through unpaired t test. All analyses were performed with Stata 13.1 (Stata Corp, College Station, Texas, USA).
Results
Nine patients with unilateral PPK were included. Five patients were female and 4 were male; in 7 cases the left eye was affected. The delay from the onset of symptoms to presentation for consultation was a median of 24 months (range 1 day to 7 years). The median age of the patients at presentation was 9 years (range 3-17 years) and the median age at the moment of the PPK was 14 years (range 7-17 years). The median BCVA before the surgery was 20/400 (range 20/60 to hand motion). Corneal sensitivity was decreased in all patients. Five patients presented with interstitial keratitis and 4 with a disciform keratitis, resulting in a central scar over the visual axis in all of them. The disease was quiescent before surgery for at least 6 months in all cases. The detailed characteristics of the patients are presented in the Table .
Of the 9 eyes, 4 were considered to be inactive on arrival and remained inactive during the complete follow-up, 3 had their first episode at presentation in our institution, and 2 were considered to be a recurrence of a previous episode. For the 3 patients with the first active disease diagnosed in our center, 2 had a documented single recurrence in the follow-up (Patients 2 and 9) before surgery; therefore, from the complete group of patients, 5 eyes were of recurring nature ( Table ). Four patients had mild corneal neovascularization limited to 1 quadrant preoperatively.
| Patient | Sex/Eye Affected | Age at Presentation/Age at PK (Years) | Type of Keratitis | Status of the Disease | BCVA Previous to PK | BCVA After PK | Complications | Time of Follow-up After PK (Months) | Complete Time of Follow-up (Months) |
|---|---|---|---|---|---|---|---|---|---|
| 1 | M/R | 15/16 | Interstitial | Inactive on arrival | 20/2000 | 20/50 | None | 21.8 | 28.3 |
| 2 | M/L | 9/16 | Disciform | First episode | 20/60 | 20/40 | None | 24.2 | 111.8 |
| 3 | F/L | 6/9 | Disciform | Recurrence | 20/200 | 20/100 | Recurrence of herpetic keratitis in graft; amblyopia | 112.6 | 117.8 |
| 4 | F/R | 13/14 | Interstitial | Inactive on arrival | 20/1000 | 20/50 | None | 35.2 | 53.9 |
| 5 | F/L | 7/7 | Interstitial | Inactive on arrival | HM | 20/400 | Amblyopia | 140.7 | 148.1 |
| 6 | M/L | 16/16 | Disciform | Recurrence | 20/400 | 20/40 | Glaucoma related to PK; required valve implant | 24.6 | 40.5 |
| 7 | M/L | 3/8 | Disciform | First episode | 20/400 | 20/30 | None | 49.1 | 94.2 |
| 8 | F/L | 17/17 | Interstitial | Inactive on arrival | 20/400 | 20/40 | None | 143.3 | 30.6 |
| 9 | F/L | 5/7 | Interstitial | First episode | HM | 20/80 | Graft rejection 15 years after PK | 190.7 | 215.1 |
No concomitant systemic diseases were found in these case series. All patients requiring a PPK received prophylactic oral acyclovir after the surgery for at least 6 months (range 6-33 months). None of these patients presented an adverse effect owing to the systemic acyclovir in the follow-up. One patient (Patient 3) presented an interstitial recurrence of HSV keratitis in the recipient cornea after interrupting prophylaxis 8 months post PPK, again requiring oral acyclovir in treatment dose; unfortunately, the recurrence led to a corneal opacity in the graft ( Figure 1 ).
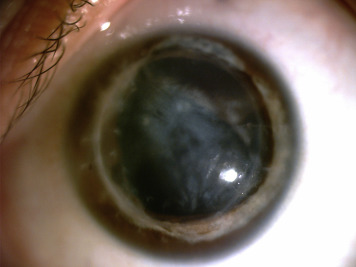
One of the patients (Patient 6) developed glaucoma 1 year after corneal transplantation, requiring a glaucoma drainage device, achieving an adequate control of the intraocular pressure after the surgery. Patient 9 presented with graft rejection 15 years after surgery, and was successfully treated with systemic acyclovir and topical corticosteroids ( Figure 2 ).




