Purpose
To estimate the probability of allograft rejection, graft failure, and recurrent keratoconus (KC) and to assess vision-specific quality of life 20 to 25 years after corneal transplantation for KC.
Design
Retrospective case series.
Methods
Two hundred nineteen eyes of 184 subjects were identified from the Michigan Corneal Transplantation Patient Registry as receiving corneal transplantation for KC from 1980 through 1986. Current ophthalmic examinations and the 25-item National Eye Institute Visual Function Questionnaire were obtained. Kaplan-Meier analyses were used to estimate the time-related probability of allograft rejection, graft failure, and KC recurrence. Cox regression was used to identify predictive factors of these outcomes. The 25-item National Eye Institute Visual Function Questionnaire scores were summarized with descriptive statistics.
Results
Follow-up was available up to 27 years after surgery (median, 10 years). Rejection occurred in 98 of 219 grafts. Most rejections occurred in the first 2 years (probability, 41%; standard error, 3%). KC recurrence was noted in 6 grafts 9 to 20 years after surgery, with a 20-year probability of 10% (standard error, 4%). Eighteen grafts failed, with a 20-year probability of 12% (standard error, 3%). Larger host trephine size, male donor gender, and nonwhite donor race were associated with increased rejection hazard. Worse astigmatism and nonwhite recipient race were associated with increased failure hazard. Twenty-eight subjects completed the 25-item National Eye Institute Visual Function Questionnaire at an average of 23 years after surgery (range, 18 to 26 years). Their mean composite score was 84.5 (standard deviation, 12.1).
Conclusions
Allograft rejection is frequent in the 2 years after corneal graft for KC. However, the 20-year probabilities of graft failure and recurrent KC are low. Given the relative youth of KC graft recipients, these statistics should enhance the information they receive.
A diagnosis of keratoconus (KC) as the primary reason for corneal transplantation long has been viewed as a positive prognostic indicator, because corneal transplantations performed for KC generally have better visual and graft survival outcomes than corneal transplantations performed for other causes. Because of this, a diagnosis of KC often is used as the basis for comparing the odds of graft survival for other common diagnoses that contribute to corneal transplantation. For example, the Singapore Corneal Transplant Study reported hazard ratios of 12.0 to 29.7 for 8 other diagnoses compared with KC in a Cox regression analysis of risk factors predictive of graft failure. A recent report from the Australian Corneal Graft Registry confirmed the advantageous survival of grafts for KC, but cautioned that their long-term survival estimates for such grafts in the typically younger KC recipients would predict the need for a repeat graft during their lifetime. For example, after 20 years of follow-up, the Kaplan-Meier estimate of survival was 49%, with a striking drop to 17% at 23 years. The goal of the current study was to estimate the likelihood of graft survival, allograft rejection, and recurrent KC, as well as vision-related quality of life, in long-term follow-up of all recipients of grafts for KC in a single United States center registry of transplantations conducted from 1980 through 1986.
Methods
This retrospective study and data collection were carried out with prospective approval from the Institutional Review Board at the University of Michigan and also were carried out in accordance with Health Insurance Portability and Accountability Act regulations. Informed consent was obtained from study participants and data were obtained under a waiver of consent when subjects could not be contacted. This study adhered to the tenets of the Declaration of Helsinki. The Michigan Corneal Transplantation Patient Registry was used to identify the records of all patients diagnosed with KC who underwent a corneal transplantation at the University of Michigan from 1980 through 1986. Preoperative and operative information was recorded for patients who underwent transplantation, including demographics (eg, age at surgery, race, gender), clinical measures (eg, best-corrected visual acuity [BCVA], concurrent ocular diseases), donor characteristics (eg, race, gender, age at donation, tissue size and quality), and surgical factors (eg, suture method, concurrent surgeries). In addition, data were obtained from annual visits after corneal transplantation, including ocular history, clinical measures, graft clarity, signs of allograft rejection, graft failure, and recurrent KC. Recurrent KC was a clinical diagnosis noted in the record by the examiner. It was based on the finding of increasing astigmatism and thinning within the donor tissue.
In an effort to obtain extended follow-up information, subjects were contacted by mail and were asked to consent to an updated eye examination at the University of Michigan Kellogg Eye Center and to complete the 25-item National Eye Institute Visual Functioning Questionnaire (NEI VFQ-25) to obtain vision-related quality-of-life information. After the mailings, subjects were contacted by phone. If the subject was willing to participate in the study, oral informed consent was obtained, and the NEI VFQ-25 was administered at this time by phone. For those who were able to come to the clinic, an eye examination was scheduled; for those who were not, an attempt was made to obtain results from their most recent visual examination from their local ophthalmologist. For patients who came to the clinic, an additional written informed consent was obtained before examination. For subjects who were unable to be contacted by phone, a chart review was conducted to obtain their most up-to-date clinical information under a waiver of informed consent.
Statistical Methods
Patient demographics, donor characteristics, and operative information were summarized using means and standard deviations (SDs) for continuous variables and frequencies and percentages for categorical variables. Kaplan-Meier analyses were used to estimate the probabilities of allograft rejection, KC recurrence, or graft failure over time from transplantation. Each eye represented an observation, and the estimates were unadjusted for correlation between bilaterally transplanted eyes. Cox regression models of time to each of these 3 events were fit to estimate the hazard ratios for various predictive factors; the sandwich estimator was used to account for correlation between eyes of a given subject. Variables investigated included patient demographics and comorbidities (age, gender, race, diabetes, and hypertension), clinical measures at the time of surgery (BCVA, average keratometry, pachymetry, astigmatism, cataract, vascularity, prior ocular surgery, and host trephine size), donor characteristics (age, gender, race, graft tissue quality, size, and endothelial cell count), and operative information (suture method, graft status, donor tissue size, and race disparity). In addition, rejection was entered as a time-dependent covariate in the Cox model for time to graft failure. Model selection was performed using the method of best subset selection, using the score statistic as the selection criterion. The proportional hazards assumption was checked by testing covariate by time interactions for each covariate. In one case of complete separation, the likelihood ratio test was used, along with the Firth adjustment of the hazard ratio. Finally, scores for the NEI VFQ-25 subscales were calculated and summarized with descriptive statistics, displayed using boxplots, and were compared between unilateral and bilaterally transplanted subjects using 2-sample t tests. All statistical analyses were performed using SAS software version 9.2 (SAS Institute, Cary, North Carolina, USA).
Results
From the Michigan Corneal Transplantation Registry, a total of 219 eyes of 184 subjects were identified as having a corneal transplant for KC. We obtained informed consent from 49 subjects, and 135 had record review conducted under a waiver of consent. Demographics, donor characteristics, and operative information are summarized in Table 1 . Subjects on average were 36.8 years of age (SD, 13.5 years; range, 15 to 103 years; n = 184) at the time of their corneal transplantation surgery, 57% (104/184) were male, and 92% (n = 170/184) were white. They were followed up for a mean of 10.6 years (SD, 7.9 years; n = 184) after transplantation. Before surgery, the average pachymetry was 0.34 mm (SD, 0.11 mm; n = 216), and deep vascularity was observed in 5% (11/219) of eyes. Donor characteristics are based on data from each corneal tissue (n = 219); some may be from the same donor, but were not linked in our database. For some variables, sample sizes are slightly reduced because of missing data. Tissue was obtained from donors who on average were 38.9 years of age (SD, 16.1 years; n = 215), and 72% (146/204) were male. A racial disparity between recipient and donor occurred in 37% (67/179) of transplants. Nearly all (99%; 178/180) donor tissue was rated good quality or better, and grafts were at least 0.5 mm larger than the host trephine size in 63% (137/219) of transplants. Of the 219 grafts, 129 (59%) were unilateral, 89 (41%) were bilateral, and 1 (< 1%) was a repeat unilateral transplant.
| Characteristics | Mean | SD | Minimum | Maximum |
|---|---|---|---|---|
| Patient characteristics (n = 184) | ||||
| Age at surgery a (y) | 36.8 | 13.5 | 15 | 103 |
| Follow-up from surgery a (y) | 10.6 | 7.9 | 0.3 | 27 |
| Frequency | Percent | |||
| Male | 104 | 56.5 | ||
| Race | ||||
| White | 170 | 92.4 | ||
| Black | 13 | 7.1 | ||
| Other | 1 | 0.5 | ||
| Diabetes | 5 | 2.7 | ||
| Hypertension | 32 | 17.4 | ||
| Mean | SD | Minimum | Maximum | |
| Preoperative recipient characteristics (n = 219 eyes) | ||||
| Pachymetry, mm (n = 216) | 0.34 | 0.11 | 0.1 | 0.9 |
| Average keratometry, D (n = 125) | 59.9 | 7.6 | 42.7 | 79.5 |
| Frequency | Percent | |||
| Deep vascularity (n = 219) | 11 | 5.0 | ||
| Prior ocular surgery (n = 219) | 15 | 6.9 | ||
| Concurrent cataract with KC (n = 219) | 21 | 9.6 | ||
| Mean | SD | Minimum | Maximum | |
| Donor characteristics (n = 219 corneas) | ||||
| Age (y; n = 215) | 38.9 | 16.1 | 2 | 70 |
| Endothelial cell count (n = 170) | 2872.7 | 445.5 | 1700 | 4666 |
| Frequency | Percent | |||
| Male (n = 204) | 146 | 71.6 | ||
| Race (n = 179) | ||||
| White | 122 | 68.2 | ||
| Black | 56 | 31.3 | ||
| Other | 1 | 0.6 | ||
| Race disparity b (n = 179) | 67 | 37.4 | ||
| White recipient/black donor | 55 | |||
| Black recipient/white donor | 10 | |||
| Frequency | Percent | |||
| Operative characteristics (n = 219 eyes) | ||||
| Host size (n = 218), mm | ||||
| 7.5 or 8.0 | 47 | 21.6 | ||
| 8.5 | 163 | 74.8 | ||
| 9.0 | 8 | 3.7 | ||
| Graft size difference ≥ 0.5 mm c (n = 219) | 137 | 62.8 | ||
| Other intraocular surgery at transplantation d (n = 219) | 14 | 6.4 | ||
| Tissue quality (n = 180) | ||||
| Excellent | 30 | 16.7 | ||
| Very good | 91 | 50.6 | ||
| Good | 57 | 31.7 | ||
| Adequate | 2 | 1.1 | ||
| Graft status (n = 219) | ||||
| Unilateral (n = 129 subjects) | 129 | 58.9 | ||
| Bilateral (n = 54 subjects) | ||||
| Both eyes in study (n = 35 subjects) | 70 | 32.0 | ||
| Only second eye in study (n = 19 subjects) | 19 | 8.7 | ||
| Repeat unilateral (n = 1 subject) | 1 | 0.5 | ||
a First surgery in subjects contributing 2 eyes to the study.
b Recipient/donor race: white/white (n = 111); black/black (n = 1); white/black (n = 55); black/white (n = 10); other/white (n = 1); white/other (n = 1); missing (n = 40).
c Host/donor size (mm): 8/8 (n = 11); 8.5/8.5 (n = 64); 9/9 (n = 6); 7.5/8 (n = 1); 8/8.5 (n = 35); 8.5/9 (n = 99); 9/10 (n = 2).
d Cataract removal, intraocular lens removal, intraocular lens implantation, and vitrectomy.
Graft rejection was observed in 98 eyes of 86 subjects, graft failure was observed in 18 eyes of 18 subjects, and KC recurrence was observed in 6 eyes of 6 subjects. Three eyes had experienced KC recurrence that resulted in graft failure; 11 of the graft failures and 3 of the KC recurrences had experienced a previous rejection episode. One eye experienced all 3 events—rejection followed by recurrence and then graft failure—over a 9.2-year period. Figure 1 displays Kaplan-Meier plots showing the cumulative probability of each of the 3 events over time after corneal transplantation. Most graft rejections occurred in the first few years after transplantation, with the percentage of rejection at 1, 5, 10, and 20 years estimated to be 33%, 45%, 46%, and 48%, respectively. The cumulative percentage with graft failure increased gradually over time, from 1% at 1 year after corneal transplantation to 4% at 5 years, 6% at 10 years, and 12% at 20 years. KC recurrence was a relatively infrequent event, with an estimated cumulative probability of 1% at 10 years, 2% at 15 years, and 10% at 20 years after transplantation.
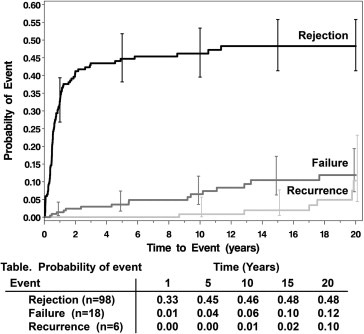
Table 2 summarizes the Cox regression model results. In a multivariate model of time to graft rejection, every 1-mm increase in the host trephine size increased the hazard of rejection 4-fold (hazard ratio [HR], 4.29; 95% confidence interval [CI], 1.58 to 11.69). Other variables predicting increased hazard of rejection were male donors (HR, 1.80 compared with female donors; 95% CI, 1.06 to 3.05) and black or other race donors (HR, 1.72 compared with white race donors; 95% CI, 1.10 to 2.67). Although first and second grafted eyes of a subject did not differ in hazard of rejection ( P = .5543), rejection events in the 2 eyes were not independent in the 35 subjects with bilateral grafts ( P = .0003), that is, those subjects were more likely to have concordant outcomes (rejections in both eyes [n = 12] or neither eye [n = 16]) than discordant outcomes (n = 7).
| Outcome | Covariates | Univariate Models | Multivariate Models | ||||
|---|---|---|---|---|---|---|---|
| HR | 95% CI | P Value | HR | 95% CI | P Value | ||
| Rejection | |||||||
| Host size (mm) a | 3.65 | 1.59 to 8.38 | .0023 | 4.29 | 1.58 to 11.69 | .0044 | |
| Male donor (vs female) | 1.68 | 1.03 to 2.73 | .0368 | 1.80 | 1.06 to 3.05 | .0285 | |
| Black/other donor (vs white) | 1.76 | 1.12 to 2.75 | .0138 | 1.72 | 1.10 to 2.67 | .0165 | |
| Failure | |||||||
| K astigmatism (for 5 diopters) | 1.57 | 1.03 to 2.40 | .0372 | 1.58 | 1.00 to 2.49 | .0502 | |
| Black/other recipient (vs white) | 4.95 | 1.49 to 16.39 | .0089 | 3.92 | 1.00 to 15.34 | .0501 | |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


