Purpose
To review presenting characteristics, clinical course, and long-term visual and anatomic outcomes of patients with traumatic macular holes at a tertiary referral center.
Design
Retrospective case series.
Methods
Twenty-eight consecutive patients with traumatic macular holes at a single tertiary referral center were reviewed. In addition to visual acuities and treatments throughout the clinical course, specific dimensions of the macular hole, including diameters, height, configuration, shape, and the presence of a cuff of fluid, were examined using spectral-domain optical coherence tomography (OCT).
Results
Twenty-eight patients were identified with a mean initial visual acuity (VA) of logMAR 1.3 (20/400) and a mean follow-up of 2.2 years. Eleven holes (39.3%) closed spontaneously in median 5.7 weeks. Eleven underwent vitrectomy with a median time to intervention of 35.1 weeks. Median time to surgery for the 5 eyes with successful hole closure was 11.0 weeks vs 56.3 weeks for the 6 eyes that failed to close ( P = .02). VA improved in closed holes ( P < .01), whether spontaneously ( P < .01) or via vitrectomy ( P = .04), but VA did not improve in holes that did not close ( P = .22). There was no relation between initial OCT dimensions and final hole closure status, although there was a trend, which did not reach statistical significance, toward small dimensions for those that closed spontaneously.
Conclusions
A fairly high spontaneous closure rate was observed, with a trend toward smaller OCT dimensions. We found no relationship between hole closure and the OCT characteristics of the hole. Surgical intervention was less successful at hole closure when elected after 3 months.
Traumatic macular holes occur in 1.4% of closed globe injuries and 0.15% of open globe injuries. They are most often associated with other retinal pathology, including commotio retinae, choroidal rupture, sclopetaria, or retinal breaks that can lead to severe vision loss.
In contrast to idiopathic macular holes, traumatic macular holes arise from a sudden extrinsic force, often blunt trauma, creating dynamic forces within the sclera and vitreous. These variable forces lead to a wide range of clinical findings in traumatic macular holes. The advent of optical coherence tomography (OCT) and its more widespread clinical use allowed for more detailed analysis of these presenting characteristics.
Huang and associates published the largest case series, reviewing the presenting OCTs of 73 traumatic macular holes. They reported average OCT measurements and configurations at presentation and compared those findings with those seen in a large series of idiopathic macular holes. However, they did not provide clinical course or OCT follow-up data on their traumatic macular hole cohort.
Smaller case series and case reports have reviewed the clinical course of those traumatic macular holes that closed spontaneously. Others have reviewed surgical outcomes in those cases that underwent vitrectomy. The largest surgical outcomes review was a multicenter trial by Johnson and associates that reviewed 25 patients who underwent vitrectomy for traumatic macular hole at 9 different centers. A meta-analysis of surgical outcomes in all published reports of vitrectomy for traumatic macular hole found a successful closure rate of 83%.
Herein, we present the largest long-term follow-up case series of consecutive traumatic macular holes at a single tertiary referral center. By reviewing both initial and follow-up OCT data, we offer new insight into the evolution of this rare but debilitating condition. Furthermore, our analysis of surgical and nonsurgical outcomes should assist retina specialists in making difficult management decisions.
Methods
This is a retrospective case series of consecutive patients with traumatic macular holes that were evaluated at the Massachusetts Eye and Ear Infirmary from July 2007 to September 2012. The study protocol was approved by the Institutional Review Board of Massachusetts Eye and Ear Infirmary (IRB protocol #12-138). The protocol allowed retrospective data collection of patients with traumatic macular holes. The study complied with the Health Insurance Portability and Accountability Act of 1996.
The type and location of the injury were recorded. Operative reports were analyzed for time to surgery and type of surgery. Visual acuity (VA) at the initial, preoperative, and final visits was recorded and converted to logMAR. Comparisons of means were conducted using the Mann-Whitney U test, paired variables were analyzed using the Wilcoxon signed rank test, and proportions were compared using the Fisher exact test. All statistical tests were 2-tailed and significance was defined as P < .05. Stata version 9.0 (StataCorp, LP, College Station, Texas, USA) was used for all statistical analyses.
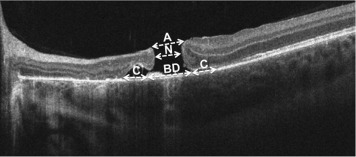
Specifics of the macular hole, such as diameter, height, configuration, and the presence of cystoid edema and subretinal fluid, were examined using spectral-domain OCT (Spectralis; Heidelberg Engineering, Heidelberg, Germany and Cirrus; Zeiss, Oberkochen, Germany). We set out to standardize the way in which macular holes are measured. In addition to the height (internal limiting membrane [ILM] to retinal pigment epithelium [RPE]), we recorded 4 specific diameters: the apical diameter, basal diameter, basal diameter including cuff of fluid, and the narrowest diameter (often considered the standard diameter OCT measurement) ( Figure 1 ).
Results
Clinical Findings
Twenty-eight patients with traumatic macular holes were identified. The mean age was 21 years and 23 (82%) were men. At presentation, 2 (7.1%) had open globe injuries, 17 (57.1%) had hyphema, 13 (46.4%) had vitreous hemorrhage, 1 (3.6%) had a posterior vitreous detachment (PVD), and 10 (38.5%; 10 of 26 with a view and records) had foveal commotio. Three patients had choroidal rupture, with only 1 involving the hole. Mean follow-up was 2.2 years. Mean initial VA was logMAR 1.3 (20/400).
Optical Coherence Tomography Characteristics at Presentation
Twenty eyes out of the 28 were imaged by OCT early in their clinical course. Their OCTs were reviewed. Seven of these OCTs were recorded only on paper printouts; thus detailed measurements were not included, although we do report their qualitative characteristics. For the remaining 13 eyes, several OCT measurements were recorded, including height, diameter (in 4 dimensions: basal, basal with cuff of fluid, apical, narrowest), shape (circular or eccentric), presence of a cuff of fluid, and configuration (flat or flap) for each hole. The average OCT measurements were as follows: basal diameter 1027 μm, basal diameter including cuff of fluid 1288 μm, narrowest diameter 283 μm, apical diameter 487 μm, and height 268 μm ( Figure 2 ). OCT confirmed that there was only 1 PVD at presentation.
Hole Closure
Eleven of the 28 holes closed spontaneously (39.3%) (median 5.6 weeks, range 1.7–67.3 weeks). All but 2 of these spontaneous closures occurred by 11 weeks, with only 1 occurring greater than 4.5 months after presentation. The mean age of those patients that had their macular holes close spontaneously was 17.6 years (range 11–26 years), whereas the mean age of those whose holes did not close was 23.5 (range 10–60 years) ( P = .359). The spontaneous closure rate was greater in children (<18 years old), at 50.0% (7/14), than in adults, at 28.6% (4/14), but did not reach statistical significance ( P = .440).
Eleven patients elected to undergo vitrectomy. Median time to intervention was 35.1 weeks. Five of 11 patients had successful closure. Median time to surgery was 11.0 weeks for the 5 eyes with successful hole closure and 56.3 weeks for the 6 eyes with holes that failed to close ( P = .017). All patients without a prior PVD had intraoperative induction of a PVD. Ten had epiretinal membrane peeling, with 8 of these also having the ILM peeled. During membrane peeling, triamcinolone, in 5 cases, and indocyanine green (ICG), in 2 cases, were used to assist visualization. Gas was used in 10 cases (90.9%), with silicone oil tamponade employed in the other case. There were no trends in surgical success among these varying surgical techniques.
Six patients did not receive intervention and their holes remained open. Two declined surgical intervention, 2 had surgery deferred owing to the presence of foveal commotio and then ultimately declined repair, and 2 were lost to follow-up after extended observation of at least 1 year.
Visual Outcomes
For all 28 eyes in our study, the VA improved overall from median logMAR 1.15 to 0.7 at the final follow-up visit ( P < .001). The VA did not improve in holes that did not close ( P = .694). In the 16 eyes with holes that closed, the VA improved from median logMAR 1.3 to 0.42 ( P < .001). In the 11 eyes with spontaneous hole closure, the VA improved from median logMAR 1.3 to 0.3 (P = .003). In the 11 eyes that underwent vitrectomy, the VA improved from median logMAR 1.2 to 0.8 ( P = .016), with the 5 that closed surgically achieving VA improvement from median logMAR 1.6 to 0.6 ( P = .043). In the holes that closed, those with an intact ellipsoid zone (EZ) band by OCT had a trend for better final visual acuity ( P = .067). Among all patients, there was no difference in final visual acuity whether or not the patient had foveal commotio at presentation (median 0.65 vs 0.65, P = .918).
Predictive Value of Optical Coherence Tomography
There was no relation between the initial dimensions of all traumatic macular holes and final closure status ( Table ). There was also no relation to hole closure if holes were classified according to shape (circular vs eccentric, P = .666), configuration (flat vs flap, P = .666), and presence or absence of a cuff of fluid ( P = .384).



