and Charles P. Molumi2
(1)
University of Papua New Guinea and Port Moresby General Hospital, Boroko, National Capital District, Papua New Guinea
(2)
Port Moresby General Hospital, Boroko, National Capital District, Papua New Guinea
8.1 Repair of Lip Defect with Abbe-Estlander Flap

Fig. 8.1
The axial flap consists of skin, muscle and mucous membrane based on superior labial artery. It is used to reconstruct one-third of the excised lower lip. A ‘v’ shaped area of excision is marked out with 1 cm of normal tissue on either side of the squamous cell carcinoma in the lower lip. Similarly an equal triangular area is marked out in the upper lip whose length is equal to the half of the defect. The vermilion border of the lips also marked

Fig. 8.2
The pedicle of the flap is based medially and it contains the superior labial artery which runs 5 mm above the upper margin of the upper lip. Buccal aspect of the tumor shows minimal extension
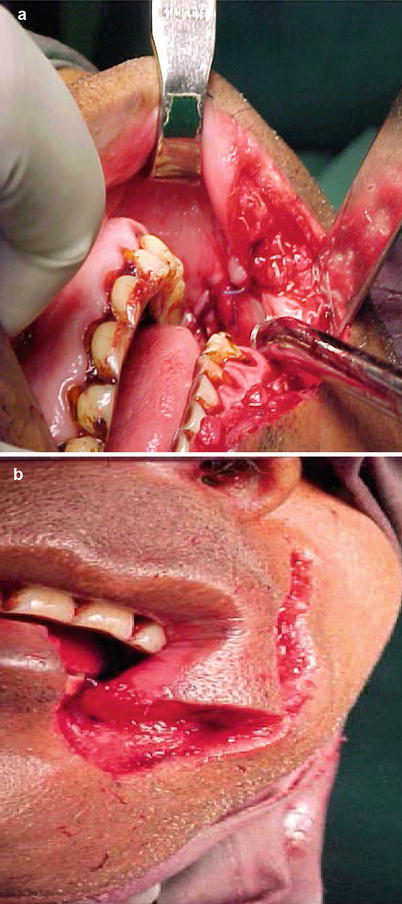
Fig. 8.3
(a, b) Using a sharp cut, the tumor is excised. The medially based flap is designed, mobilized and rotated into the defect, and sutured in place in three layers, skin, muscle and mucosa

Fig. 8.4
The donor area is mobilized and closed in three layers. The lip commissure is formed in the process of flap rotation. The cut ends of the lip is sutured

Fig. 8.5
After 4 weeks the wound heals with less scaring. The scar is eventually indistinguishable
8.2 Repair of Full Thickness Lip Defect

Fig. 8.6
Full length mucosal lesion of the lower lip with cutaneous infiltration in the midline is marked out for excision

Fig. 8.7
The mucosal lesion is excised with a ‘V’ shaped cutaneous and mucosal incision in the midline

Fig. 8.8
The defect of the lip after excision

Fig. 8.9
The closure of the surgical defect is begun by placing sutures through the vermillion edge of the skin of the ‘V’ shaped defect for accurate approximation

Fig. 8.10
The skin, muscle and mucosal layers of the ‘V’ shaped defect is sutured

Fig. 8.11
The skin to mucosa of the lip margins are approximated
8.3 Repair of Near Total Lop Defect by Karapandzic Flap

Fig. 8.12
Full thickness of the lower lip involved by exophytic squamous cell carcinoma

Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


