The lip is an important functional and esthetic facial feature used for relatively simple tasks, such as retaining oral contents, as well as for complex functions, such as smiling, kissing, and expressing emotion. Like the eyes, the lips have a defining role in the concept of modern beauty not only in Western culture but also in others. From the Surma women of Ethiopia who stretch their lips with successively larger plates to advertise their dowries to the Western obsession with full lips, as evidenced by the popularity of lip augmentation, the lip has a vital role in facial esthetics.
Function, of course, follows form. The lips function as a sphincter for retaining oral contents during mastication. They are integral during phonation of certain sounds, such as the letters “M,” “B” and “P.” The lip has a central role in the expression of emotion. The smile on Mona Lisa’s lips has beguiled men for centuries.
This article is devoted to details of the anatomy, pathology, presurgical considerations, and specific techniques used in reconstructing the lip. A general algorithm to lip reconstruction is outlined. The repair of superficial lesions is considered first, followed by a discussion of lower lip defects in order of increasing size and complexity. Some of the special considerations associated with repair of the upper lip and commissure are explained.
Anatomy
Facial development starts in the early embryonic period. The mandible and maxilla are derived from the first pharyngeal arch. The upper lip develops from the fusion of the maxillary and medial nasal prominences and the intermaxillary segment. The commissure is formed by the fusion of the lateral portion of the maxillary processes with the mandibular processes. The lower lip and mandible are derived from the mandibular process, which develops as a single structure that crosses the midline. The embryology of the lip has pathologic and functional implications. Cleft lip results from dysfunctional development of the upper lip. The embryologic boundary between the left and right upper lip causes lymphatic drainage to occur ipsilaterally. The lower lip has no such boundary and can drain bilaterally to cervical lymph nodes.
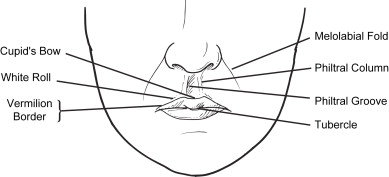
The lip encompasses the area from the subnasale to the mental crease and from commissure to commissure ( Fig. 1 ). The skin and vermilion are separated by a paler rim of tissue called the white roll. The red line separates the “dry” vermilion from the intraoral labial mucosa, also known as the “wet” lip. The vermilion contains no sweat glands or hair follicles and is comprised of keratinized stratified squamous epithelium that overlies a highly vascular bed of tissue that gives the lips their rosy hue. The upper lip is shaped like an elongated M, the apices of which form the lower extent of the philtral columns. The apices of the upper lip along with the central depression are referred to collectively as Cupid’s bow. The tubercle is the prominence in the center of the upper lip. The philtral columns extend up to the columella and are separated by the philtral groove. Once damaged, they are difficult to reconstruct. The upper lip is divided into three esthetic subunits: the central philtrum and the paired lateral units spanning from the philtral columns to the melolabial folds. Relaxed skin tension lines are oriented radially around the mouth. The complex and elegant landmarks within and around the upper lip make reconstructing this region a challenge.
The lower lip is considerably more straightforward than the upper lip in terms of surface anatomy. It is slightly shorter than the upper lip and varies in width along its length. The mental crease demarcates the border between the lip and chin and corresponds to the lowest extent of the gingival sulcus. Incisions that cross the mental crease have a tendency to form hypertrophic scars.
The musculature of the lip is complex, including the orbicularis oris plus more than a dozen paired muscles whose actions are elevation, depression, and sphincteric . The modiolus is a fibrous structure anchored to the deep layers of skin at the corner of the mouth that serves as the origin or insertion of many of the perioral muscles.
The orbicularis oris makes up the bulk of the tissue of the lip and acts as the sphincter muscle to the oral aperture. The deep fibers of the orbicularis oris are oriented horizontally and act to compress the lips and provide sphincter function, whereas the superficial fibers are responsible for finer movements. Intermingled with the horizontal fibers are oblique fibers that act to evert the lips, giving them their characteristic pout in profile. The resting tone in the orbicularis oris muscle can make defects of the lip appear larger than they actually are by pulling on wound edges; this effect should be taken into consideration when planning a repair. The depressors of the lip include the depressor anguli oris, depressor labii inferioris, and the platysma. Elevators of the lip include the levator labii superioris, zygomaticus, risorius, and mentalis.
Sensory innervation to the upper lip is via the infraorbital branch of the trigeminal nerve. The mental branch of the trigeminal nerve provides sensory innervation to the lower lip. Both of these nerves are easily blocked peripherally, allowing for minor procedures under local anesthesia. Motor innervation to the muscles of the lips is via the buccal and marginal mandibular branches of the facial nerve. Nerves enter deep to the muscles with the exception of the mentalis muscle, which receives its innervation superficially from the marginal mandibular nerve.
Marginal mandibular nerve palsy can cause the affected side of the mouth to have an elevated lower lateral lip secondary to loss of function of the depressor anguli oris and depressor labii inferioris.
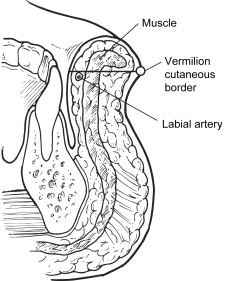
The blood supply to both lips is derived from the facial artery via the superior and inferior labial branches. The labial arteries are consistently located between the orbicularis oris and the mucosal surface of the lip, near the free edges of the lips ( Fig. 2 ). Venous drainage generally runs with the arteries; however, the upper lip can drain via the ophthalmic vein to the cavernous sinus, providing a route for labial infections to spread intracranially.
Pathology
Neoplastic disorders make up the majority of lip pathology encountered by surgeons, but other disease processes, trauma, and burns can involve the lip and require surgical repair. Squamous cell carcinoma is the most common malignancy affecting the lip, unlike the remainder of the facial skin where basal cell carcinomas predominate. Risk factors for squamous cell carcinoma include male gender, sun exposure, tobacco use, and fair complexion. Because the lower lip receives more ultraviolet exposure than does the upper lip, 90% of all squamous cell carcinomas occur here. Carcinomas originating from the upper lip and commissure are generally considered more aggressive than carcinomas arising from the lower lip. Actinic cheilitis is a precursor lesion to squamous cell carcinoma that presents with hyper-keratosis, desquamation, and crusting. Bleeding and erosions are signs of more advanced disease. Treatment for this premalignant condition can be with topical antineoplastic creams, CO 2 laser ablation, or surgical vermilionectomy, depending on the extent of disease and patient preference .
Other malignancies affecting the lip include basal cell carcinoma, melanoma, microcystic adnexal carcinoma, and Merkel cell carcinoma. Malignant melanoma presents on the lips most frequently as a pigmented lesion, although amelanotic melanomas occur as well. Microcystic adnexal carcinoma originates from sweat ducts and generally presents as a yellow plaque or nodule on the upper lip. It is known for perineural invasion causing numbness and par-esthesias, and tends to be locally invasive with a high rate of recurrence. Merkel cell carcinoma is derived from neural crest cells and is characterized by rapid growth, a high rate of local recurrence, and nodal and distant metastases at the time of diagnosis.
The lip may be involved in many other disease processes, such as granulomatous cheilitis, heman-giomas, nevi, labial melanotic macules, and infectious processes such as noma, a destructive fasciitis that occurs in malnourished persons. Trauma to the lip occurs frequently and from a multitude of causes, including automobile accidents, interpersonal violence, animal bites, and electrical burns. Determining the mechanism and timing of injury is important when planning treatment, because infection and surrounding soft tissue injury must be considered.
Pathology
Neoplastic disorders make up the majority of lip pathology encountered by surgeons, but other disease processes, trauma, and burns can involve the lip and require surgical repair. Squamous cell carcinoma is the most common malignancy affecting the lip, unlike the remainder of the facial skin where basal cell carcinomas predominate. Risk factors for squamous cell carcinoma include male gender, sun exposure, tobacco use, and fair complexion. Because the lower lip receives more ultraviolet exposure than does the upper lip, 90% of all squamous cell carcinomas occur here. Carcinomas originating from the upper lip and commissure are generally considered more aggressive than carcinomas arising from the lower lip. Actinic cheilitis is a precursor lesion to squamous cell carcinoma that presents with hyper-keratosis, desquamation, and crusting. Bleeding and erosions are signs of more advanced disease. Treatment for this premalignant condition can be with topical antineoplastic creams, CO 2 laser ablation, or surgical vermilionectomy, depending on the extent of disease and patient preference .
Other malignancies affecting the lip include basal cell carcinoma, melanoma, microcystic adnexal carcinoma, and Merkel cell carcinoma. Malignant melanoma presents on the lips most frequently as a pigmented lesion, although amelanotic melanomas occur as well. Microcystic adnexal carcinoma originates from sweat ducts and generally presents as a yellow plaque or nodule on the upper lip. It is known for perineural invasion causing numbness and par-esthesias, and tends to be locally invasive with a high rate of recurrence. Merkel cell carcinoma is derived from neural crest cells and is characterized by rapid growth, a high rate of local recurrence, and nodal and distant metastases at the time of diagnosis.
The lip may be involved in many other disease processes, such as granulomatous cheilitis, heman-giomas, nevi, labial melanotic macules, and infectious processes such as noma, a destructive fasciitis that occurs in malnourished persons. Trauma to the lip occurs frequently and from a multitude of causes, including automobile accidents, interpersonal violence, animal bites, and electrical burns. Determining the mechanism and timing of injury is important when planning treatment, because infection and surrounding soft tissue injury must be considered.
General concepts in lip repair
Functional and cosmetic considerations are paramount when planning the repair of a lip defect. The lip has several important functions, including retaining oral contents, phonation, and allowing passage of objects into the oral cavity, such as dentures. Micro-stomia is an important complication of lip repair that can hinder oral hygiene and the use of dentures. Occasionally, it is necessary to bring new tissue into the lip to prevent microstomia. Figs. 3 and 4 outline a basic approach to reconstructing the lip.
The basic principles of wound closure apply to repairs of the lip. Careful evaluation, debridement, hemostasis, alignment of the vermilion border, and a thorough approximation of the muscular layer are the keys to a functionally and esthetically pleasing result. Ideally, one must realign all muscle fibers along their original direction and preserve lip height. Unrepaired muscular defects can contract during the healing process and create a visible notch along the wet lip border.
Topographic boundaries and esthetic units of the lip must be recognized and respected when planning a surgical repair. It is prudent to mark important structures before the injection of any local anesthetic, especially the vermilion border and white roll. Even small discrepancies within these important landmarks are obvious to a casual observer. The melolabial fold, mental crease, and philtral ridges are esthetic subunit boundaries of the lip region that are useful for camouflaging scars. It is best to avoid crossing these boundaries. When a defect takes up a substantial portion of an esthetic subunit, replacement of the entire subunit may provide the best cosmetic result. The relaxed skin tension lines and facial wrinkles run parallel in the perioral region and generally perpendicular to the vermilion. Vertical scars are favorable for these esthetic reasons, as well as the fact that they tend to maintain lip height.
In general, muscle and subcutaneous fascia should be closed with a long-acting absorbable suture, the intraoral mucosa with a more rapid-absorbing material such as catgut, and the vermilion with a soft permanent suture such as silk (to be removed after 5–7 days).
Superficial defects
Some small defects of the lip or vermilion that do not involve the underlying orbicularis muscle may heal nicely through second intention . Wound contracture must be anticipated, because even small notches along the lip border can be disfiguring. Full-thickness skin grafts and local transposition flaps remain a workhorse for smaller cutaneous defects, particularly of the upper lip. The cheek can be an excellent source for adjacent tissue recruitment while leaving the essential landmarks of the perioral area undisturbed ( Fig. 5 ). The underlying muscle can begin to bunch up with flap rotation and may require gentle debulking to preserve a natural lip contour. Larger cutaneous flaps can quickly distort the area. Superficial defects are often converted to full-thickness ones and repaired with composite myocuta-neous flaps.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


