Limbal Stem Cell Transplantation
Erik Letko
C. Stephen Foster
The objective of limbal stem cell transplantation is to restore the corneal surface with normal corneal epithelium. Normal corneal epithelium is maintained in the state of homeostasis by balancing epithelial shedding from the surface with centripetal movement of stem cell-derived epithelial cells from the limbus and proliferation of the basal cells (1,2). This so-called XYZ hypothesis of Thoft and Friend, where X represents proliferation of basal cells, Y proliferation and centripetal migration of limbal cells, and Z represents epithelial cell loss from the surface of the cornea, was first proposed in 1983 (3). Cotsarelis et al. were the first to report on the existence of slow-cycling corneal epithelial cells located in the basal cell layer of the limbus (2). These cells were later referred to as corneal limbal stem cells.
The limbal stem cells have several distinct biologic and morphologic characteristics. Their life span is believed to be lifelong. They do not have direct cell-to-cell communication by gap junctions and therefore they must maintain a distinct intracellular environment with a substantial degree of metabolic autosufficiency that enables them to survive isolated from their neighbors (4). The absence of expression of the cornea-specific 64-kD protein K3 and expression of keratin-19 are unique features of limbal stem cells. The stem cells have a capacity to self-renew and generate transient amplifying cells that are positioned in the basal cell layer of the corneal epithelium. Unlike suprabasal corneal epithelial cells, both stem cells and transient amplifying cells are characterized by prolonged retention of H-labeled thymidine under stimulation by a tumor promoter (1,2,5). The transient amplifying cells maintain a high capacity for proliferation, but unlike stem cells, their life span is reduced to several months. Stem cells and transient amplifying cells form the proliferative tissue compartment (6). The remaining corneal epithelial cells, located in suprabasal layers, are terminally differentiated cells with a life span of approximately 1 week. Unlike limbal grafts that contain stem cells, penetrating and lamellar corneal grafts contain only transient amplifying and terminally differentiated cells (7). Limbal epithelial cells (but not conjunctival epithelial cells) inhibit fibroblast-stimulated angiogenesis and may therefore play a role in the maintenance of corneal avascularity (8).
Corneal surface reconstruction by transplanting a graft from other ocular surface epithelium was first reported in 1977 by Thoft, who used autologous contralateral conjunctiva in patients with severe unilateral alkali burn (9). Six years later, Thoft proposed transplantation of limbal corneal epithelium from fresh cadaver eyes and called this procedure keratoepithelioplasty (10). Kenyon and Tseng then described a series of patients with “limbal stem cell transplantation” in 1989 (11), and since then, many others have used this procedure successfully in patients with a spectrum of disorders characterized by limbal stem cell deficiency (Table 59-1).
Limbal stem cell deficiency can present with clinical signs of persistent corneal epithelial defect, neovascularization, “conjunctivalization,” scarring, stromal ulcer, calcification, and band keratopathy (12, 13, 14, 15, 16, 17). The most common symptoms of limbal stem cell deficiency are decreased vision, photophobia, tearing, blepharospasm, recurrent pain, and redness.
Chronic inflammation of the conjunctiva, conjunctival scarring, symblepharon formation, trichiasis, distichiasis, meibomian gland dysfunction, and lacrimal gland inflammation are all factors that can lead to tear film abnormalities and ultimately to damage to limbal stem cells and corneal epithelium that can present as persistent epithelial defect, corneal scarring, and neovascularization (18). These factors can compromise limbal stem cells and exacerbate limbal stem cell insufficiency. Therefore, they need to be identified and eliminated to the maximum possible extent before limbal stem cell grafting to increase the graft survival time. The data indicating that success rates of limbal stem cell transplantation performed several months after burn injury may be higher compared with earlier transplantation (19) further support the idea that limbal stem cell transplantation in inflamed eyes should be avoided.
TABLE 59-1. INDICATIONS FOR LIMBAL STEM CELL TRANSPLANTATION | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
SURGICAL TECHNIQUE AND PERIOPERATIVE MANAGEMENT
Chronic inflammation of the conjunctiva, conjunctival scarring, symblepharon formation, trichiasis, distichiasis, meibomian gland dysfunction, and lacrimal gland inflammation are all factors that can lead to tear film abnormalities and ultimately to a damage to limbal stem cells and corneal epithelium that can present as persistent epithelial defect, corneal scarring and neovascularization (18). These factors can compromise limbal stem cells and exacerbate limbal stem cell insufficiency. Therefore, such factors must be identified and eliminated to the maximum possible extent prior to limbal stem cell grafting; otherwise, the grafted tissue will be damaged and will probably not survive. The data indicating that success rate of limbal stem cell transplantation performed several months after burn injury may be higher compared to earlier transplantation (19) further support the idea that limbal stem cell transplantation in inflamed eyes should be avoided.
After peribulbar anesthesia, a 360-degree peritomy is performed on the recipient eye. Abnormal epithelium is removed from the cornea, and a superficial keratectomy is performed to ensure a smooth surface.
Attention is then paid to the donor eye. After peribulbar anesthesia, a 15 degree supersharp blade is used to outline the corneal portion of donor lenticle approximately 1 mm from the limbus and spanning 2 clock hours circumferentially. Vannas scissors are used to dissect the conjunctival portion of the lenticle, approximately 2 mm posterior to the limbus. One edge of the lenticle is lifted with forceps and dissected, as a lamellar dissection, from its remaining attachment at the limbus and cornea, and the donor graft is immediately placed in balanced salt solution. After harvesting one to three lenticles (a maximum of 6 clock hours), an antibiotic and steroid ointment is applied onto the surface of the donor eye and the eye is pressure patched until the following day.
The donor lenticles are then placed onto the limbal area of the recipient eye and secured to the cornea with 10-0 nylon sutures and to the episclera using 10-0 polyglactin sutures. An amniotic membrane graft may be placed to cover the entire corneal surface at the surgeon’s discretion and sutured to the episclera and conjunctiva with 10-0 polyglactin sutures. An 18-mm hydrophilic bandage contact lens is placed onto the ocular surface at the end of the procedure.
Topical steroids and antibiotics are applied regularly in the postoperative period. The antibiotic drops are discontinued after the epithelium has healed and the bandage contact lens has been removed. The steroid drops, administered every hour for the first week after surgery, are tapered gradually and discontinued when inflammation has subsided. Systemic immunosuppressive therapy to prevent graft rejection is indicated in patients with limbal stem cell allograft. Additional use of autologous serum drops in the postoperative period may enhance corneal reepithelialization (20) (Fig. 59-1).
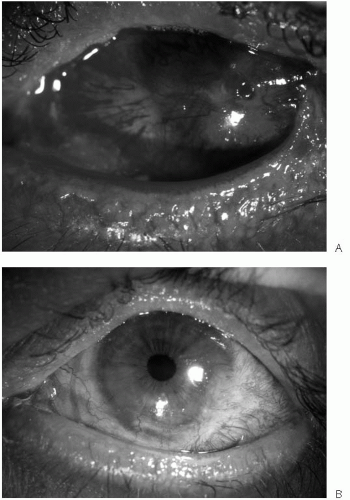 FIGURE 59-1. A patient with history of toxic epidermal necrolysis before (A) and 6 months after (B) limbal stem cell allotransplantation.(see color image) |
COMPLICATIONS
Limbal stem cell transplantation has an excellent safety record. Only scattered intraoperative and postoperative complications have been reported. Immune rejection reaction and limbal stem cell graft failure are the most common postoperative complications in the recipient eye. Increased intraocular pressure after limbal stem cell transplantation, believed to be related to the use of steroids in the postoperative period, was reported in up to 37% of patients after limbal stem cell transplantation (21). This observation suggests an early institution of steroid-sparing therapy to prevent the immune rejection reaction. An infectious keratitis complicating the postoperative period may compromise limbal stem cells and lead to a permanent limbal stem cell failure (22). Corneal epithelial cells differentiated from donor-derived limbal stem cells repopulate the corneal surface after limbal stem cell transplantation (23). Donor-derived epithelial cells are present on the corneal surface much longer after limbal stem cell transplantation than after penetrating keratoplasty alone (23). The size of the donor graft may play a role in graft sufficiency (24). Although reepithelialization of the corneal surface with total limbal stem cell deficiency can occur with limbal stem cell grafts 5 mm long or smaller (24), these grafts are less efficient than 7- to 10-mm limbal grafts (24,25). However, even with larger limbal grafts, graft function can be compromised over time (26,27). The duration of postoperative limbal stem cell survival is limited by several factors, such as persistent inflammation, dry eye, and progressive rejection of the limbal stem cell graft (28). A limbal stem cell graft is considered to have failed if signs of stem cell deficiency are present.
Few cases of intraoperative or postoperative complications have been reported in donor eyes. These include microperforation (29), donor filamentary keratitis (30), epitheliopathy in a patient with history of contact lens wear (31), pseudopterygium (32,33), “abnormal epithelium” (25), and “corneal depression” (34).
AUTOLOGOUS LIMBAL STEM CELL TRANSPLANTATION
Autologous limbal stem cell grafts can be used in patients with unilateral limbal stem cell deficiency or in patients with limbal stem cell deficiency limited to a small portion of the limbus (e.g., pterygium). The autologous graft can be obtained either from the healthy fellow eye or from the affected eye. The choice of donor eye is made according to the extent and etiology of limbal stem cell deficiency. Three clock hours of limbal stem cell autograft were successfully removed and transplanted to a different area of the limbus of the same eye in a patient with recurrent pterygium (30) (Fig. 59-2). The major advantage of autologous grafting is avoidance of immunosuppressive therapy to prevent the immune rejection reaction. When total limbal stem cell deficiency is present only in one eye, limbal stem cell grafts can be obtained from the fellow eye (11).
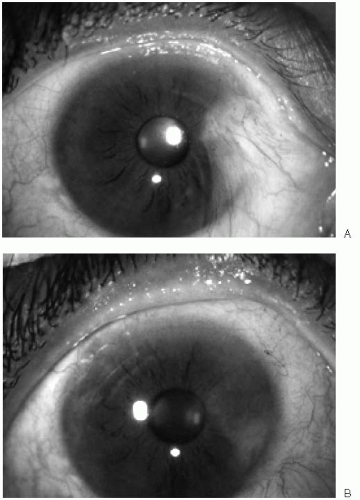 FIGURE 59-2. A patient with recurrent pterygium before (A) and 6 months after (B) limbal stem cell autotransplantation from the same eye. |
ALLOGENIC LIMBAL STEM CELL TRANSPLANTATION
If limbal stem cell deficiency involves both eyes, corneal surface reconstruction depends on an allogenic source of limbal stem cells. The allogenic graft can be obtained either from living donors (35,36) or from cadaveric donors (20,25,35,37). It is generally accepted that harvesting of up to 6 clock hours of limbal stem cells is considered to be safe in a normal, healthy living donor eye. Special attention needs to be paid to the donor eye during the preoperative slit-lamp examination. Subtle signs such as alteration or loss of palisades of Vogt from the inferior limbus may be indicative of damage to the limbus (14). Preoperative
impression cytology of the donor corneal epithelium is recommended in cases suspect for limbal stem cell deficiency (19). The presence of goblet cells on the cornea is a sign of compromised limbal stem cell function, and harvesting limbal stem cells from such a donor eye should be avoided (38). The advantage of using a cadaver donor eye is that all limbal stem cells can be harvested.
impression cytology of the donor corneal epithelium is recommended in cases suspect for limbal stem cell deficiency (19). The presence of goblet cells on the cornea is a sign of compromised limbal stem cell function, and harvesting limbal stem cells from such a donor eye should be avoided (38). The advantage of using a cadaver donor eye is that all limbal stem cells can be harvested.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


