Purpose
To describe the outcomes of limbal stem cell transplantation in eyes with limbal stem cell deficiency related to soft contact lens wear.
Design
Retrospective interventional case series.
Methods
Institutional database search at the Cincinnati Eye Institute revealed 9 patients (14 eyes) who underwent limbal stem cell transplantation with systemic immunosuppression for soft contact lens wear–related limbal stem cell deficiency. Outcome measures included patient demographics, symptoms, best-corrected visual acuity, ocular surface stability, adverse events, and additional surgeries required.
Results
Average patient age at time of surgery was 46.6 ± 11.1 years (range 20–60 years). Average duration of follow-up was 28 ± 19.1 months (range 12–70 months). Preoperative best-corrected visual acuity (BCVA) was 20/40 or worse in all eyes (average 20/70, range 20/40–20/250) and patient symptoms included foreign body sensation, tearing, redness, and/or pain. Four eyes (29%) underwent living-related conjunctival limbal allograft and 10 eyes (71%) underwent cadaver-donor keratolimbal allograft surgery. Topical and systemic immunosuppression was used in all patients. At final follow-up after limbal stem cell transplantation, there was a stable ocular surface in 12 of 14 eyes (86%) and improvement in BCVA to 20/30 or better and complete resolution of patient symptoms in all except 1 patient who had significant rosacea blepharokeratoconjunctivitis, whose BCVA remained at 20/150 and 20/60, in right and left eyes, respectively. The most common adverse event was an increase in intraocular pressure in 8 of 14 eyes (57%), requiring topical antiglaucoma treatment. Ten of 14 eyes (71%) underwent cataract extraction related to topical steroid use. No eyes required subsequent penetrating keratoplasty.
Conclusion
Limbal stem cell transplantation is a viable option for the management of soft contact lens wear–related limbal stem cell deficiency in young healthy patients. Early intervention prior to subepithelial fibrosis can lead to good visual outcomes with no need for subsequent cornea transplant. Co-management with a solid organ transplant specialist is helpful for the monitoring and management of systemic adverse events related to patient systemic immunosuppression.
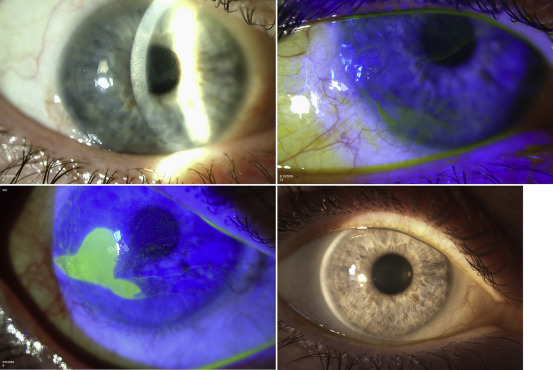
Limbal stem cells are required for the maintenance of a stable corneal epithelial surface and act as a barrier to any conjunctivalization of the cornea. The loss or dysfunction of the limbal stem cells results in limbal stem cell deficiency. Clinically, this manifests as persistent epithelial defects, corneal conjunctivalization, corneal scarring, chronic inflammation, vision loss, chronic pain, photophobia, and keratoplasty failure. On examination, the epithelium may appear opaque, and/or a classic pattern of late fluorescein corneal staining occurs ( Figure ) because of the increased permeability of abnormal epithelial cells. In addition, migrating conjunctival goblet cells can be detected on the corneal surface by impression cytology.
Numerous causes of limbal stem cell deficiency exist, including aniridia, chemical injury, burns, radiation, Stevens-Johnson syndrome, contact lens wear, and cicatricial pemphigoid, among others. Limbal stem cell deficiency can be staged according to amount of limbal involvement and the inflammatory status of the conjunctiva. Severe limbal stem cell deficiency is a rare complication of contact lens wear that has been associated with female sex and extended duration of wear time. It is classified as stage AII by a loss of limbal stem cells greater than 6 clock hours (near total) up to 12 clock hours (total). In less severe or partial contact lens wear–related limbal stem cell deficiency (stage AI), patients can be managed with conservative treatment consisting of the discontinuation of contact lens wear, management of dry eye and blepharitis, epithelial debridement and amniotic membrane graft, and/or sequential epithelial debridement. However, in severe contact lens wear–related limbal stem cell deficiency, limbal stem cell transplantation is required for restoration of the corneal phenotype. Keratolimbal allograft and living-related conjunctival limbal allograft are 2 techniques for transplanting allogenic tissue containing limbal stem cells into a recipient eye. The purpose of this study was to describe the outcomes of limbal stem cell transplantation by keratolimbal allograft and living-related conjunctival limbal allograft in the treatment of severe contact lens wear–related limbal stem cell deficiency.
Methods
This retrospective study was reviewed by the St Elizabeth’s Health Care (Edgewood, Kentucky) Institutional Review Board (IRB # 4/2011-009) and determined to be exempt. This study was conducted in compliance with the tenets of the Declaration of Helsinki.
Patients
A database search of patients with a diagnosis of severe limbal stem cell deficiency related to contact lens wear was conducted at a single institution. The charts of 18 eyes from 12 patients were identified. Of those, 14 eyes from 9 patients had undergone limbal stem cell transplantation and their charts were retrospectively reviewed.
Outcome measures that were analyzed consisted of patient demographics, presenting symptoms, change in best-corrected visual acuity (BCVA), type of limbal stem cell transplant, ocular surface stability, adverse events, and additional surgeries required. A stable ocular surface was defined as an intact corneal epithelium and absence of corneal conjunctivalization and conjunctival inflammation. An improved ocular surface was defined as a partial failure with areas of healthy cornea and areas of abnormal conjunctival epithelium.
Surgical Procedures
Keratolimbal allograft
The protocol for tissue procurement and preparation was followed, and this surgical technique has been described previously. Briefiy, paired corneoscleral rims were used as the source for transplanted limbal stem cells. The central cornea was excised with a 7.5 mm trephine. The remaining corneoscleral rim was sectioned into 2 equal halves, and excess peripheral scleral tissue was trimmed. The posterior one half to two thirds of each hemisection was removed via lamellar dissection using a steel crescent blade and then discarded. A 360-degree limbal peritomy was performed on the recipient eye. The conjunctiva was resected for 4–5 mm to expose an adequate area of sclera on which to position the allograft tissue. Abnormal fibrovascular pannus and epithelium were removed from the cornea with a combination of sharp and blunt dissection. Three of the 4 dissected crescents were placed on the recipient eye with the donor corneal edge overlying the recipient limbus secured with 10-0 nylon interrupted buried sutures and with tissue glue for the base. The recipient conjunctival edge was ensured to abut the posterior edge of the transplanted tissue.
Living-related conjunctival limbal allograft
The protocol for tissue procurement and preparation was followed, and this surgical technique has been described previously. Briefly, the best match from potential donors was identified from immediate relatives based on human leukocyte antigen and ABO blood typing. Donors were assessed preoperatively for transmissible diseases and to ensure there were no ocular pathologic conditions present. The nondominant eye was selected as the donor.
In the donor eye, 3 clock hours of limbal conjunctival tissue at the 12- and 6-o’clock positions were marked with a gentian violet blue marker and resected 3–4 mm posteriorly. Conjunctival tissue, including the Vogt palisades, was dissected 1 mm anteriorly onto the corneal surface. Vannas scissors were then used to cut the conjunctiva from the cornea. The 2 pieces of donor tissue were floated on balanced salt solution (Alcon, Fort Worth, Texas, USA) and transferred for transplantation to the recipient. The conjunctival wounds were then closed 1 mm posterior to the limbus using 10-0 vicryl sutures (Ethicon, Johnson & Johnson, Cincinnati, OH). Subconjunctival injections of ancef and dexamethasone were given. A topical-fourth generation fluoroquinolone was applied and the eye was patched.
In the recipient, a conjunctival peritomy was performed at the 12- and 6-o’clock positions, and limbal conjunctiva was undermined and allowed to retract posteriorly. Removal of pannus and irregular epithelium was performed by debridement and careful dissection using a 64 blade. The conjunctival-limbal grafts were secured at the limbus using 10-0 nylon sutures and at the base with tissue glue. Subconjunctival injections of cefazolin and dexamethasone were administered. A large-diameter contact lens was placed and a patch applied.
Immunosuppression Regimen
All patients received an immunosuppression regimen as previously described. In brief, postoperatively, patients were given topical cyclosporine 0.05% 2 times daily and prednisolone acetate or difluprednate 1% 4 times daily. Topical steroid was maintained at 4 times daily for the first 3 months and then decreased by 1 drop per month. Patients were then maintained on topical steroids at least once daily according to the degree of conjunctival inflammation.
Systemic immunosuppression generally consisted of prednisone 1 mg/kg per day for 1 month, then tapered for both living-related and keratolimbal allografts; oral tacrolimus 4 mg twice daily, then tapered after 1 year for living-related and after 2 years for keratolimbal allografts; and mycophenolate mofetil 1 g twice daily, then tapered after 6–12 months for living-related and 2–3 years for keratolimbal allografts. Regimens were initiated 2 weeks prior to surgery and tailored according to the degree of conjunctival inflammation. Valganciclovir 225 mg daily for 1 year (discontinued if CMV IgG negative) and sulfamethoxazole and trimethoprim 1 tablet 3 times weekly were given as prophylaxis.
Statistical Analysis
BCVA was converted from measured Snellen values to logarithm of the minimal angle of resolution (logMAR) for statistical analysis and averages were converted back to Snellen to be reported in the results. Distribution of data was assessed for normality using the Shapiro-Wilk test. Postoperative BCVA failed to demonstrate normality. Nonparametric Wilcoxon paired signed rank test was subsequently used to compare preoperative and postoperative logMAR values.
Results
Results are summarized in the Table . The average age at diagnosis was 45.6 ± 10.9 years (range 19–58 years) and the average age at surgery was 46.6 ± 11.1 years (range 20–60 years). Eight right eyes and 6 left eyes were included. Most patients (67%; 6/9) were female and all patients wore soft contact lenses only.
| Eye No. | Patient No. | Age at Surgery (y) | Sex | Eye | # Clock Hours of Conjunctivalization (Location) | Prior Treatments | Preoperative BCVA | Surgery | Follow-up (mo) | Postoperative BCVA | Symptom Resolution | Side Effects Related to Systemic Immunosuppression | Systemic Immunosuppression at Last Follow-up | Other Surgery |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 1 | 28 | M | OD | 12 (Total) | Doxycycline | 20/40 | LR-CLAL | 12 | 20/30 | Complete | Mycophenolate mofetil + tacrolimus | ||
| 2 | 2 | 20 | M | OS | 12 (Total) | Lotemax, vitamin A ointment | 20/250 | KLAL | 12 | 20/20 | Complete | Hyperbilirubinemia | Mycophenolate mofetil + tacrolimus | |
| 3 | 3 | 44 | F | OD | 12 (Total) | Superficial keratectomy, phototherapeutic keratectomy, Pred forte | 20/200 | LR-CLAL | 21 | 20/30 | Complete | Neutropenia | Mycophenolate mofetil | |
| 4 | 3 | 44 | F | OS | 6 (Superior) | Superficial keratectomy, phototherapeutic keratectomy, Pred forte | 20/40 | LR-CLAL | 18 | 20/20 | Complete | Neutropenia | Mycophenolate mofetil | |
| 5 | 4 | 50 | F | OS | 12 (Total) | Meibomian gland dysfunction | 20/70 | KLAL + lateral tarsorrhaphy | 70 | 20/30 | Complete | None | Phaco, IOL | |
| 6 | 4 | 50 | F | OD | 12 (Total) | Meibomian gland dysfunction | 20/80 | KLAL + lateral tarsorrhaphy | 65 | 20/30 | Complete | None | Phaco, IOL | |
| 7 | 5 | 42 | M | OD | 12 (Total) | Lotemax, serum drops, artificial tears and ointment | 20/50 | KLAL | 28 | 20/20 | Complete | Mycophenolate mofetil | Phaco, IOL | |
| 8 | 6 | 60 | F | OS | 9 (Superior) | Vitamin A, nonpreserved artificial tears, temporal 70% lateral tarsorrhaphy for persistent epithelial defect | 20/70 | KLAL | 33 | 20/25 | Complete | Nausea | Mycophenolate mofetil | Phaco, IOL |
| 9 | 6 | 60 | F | OD | 6 (Superior) | Vitamin A ointment | 20/30 | KLAL | 18 | 20/20 | Complete | Nausea | Mycophenolate mofetil | Phaco, IOL |
| 10 | 7 | 58 | F | OD | 12 (Total) | Vitamin A ointment | 20/60 | LR-CLAL | 17 | 20/25 | Complete | Mycophenolate mofetil | Phaco, IOL | |
| 11 | 8 | 50 | F | OS | 12 (Total) | 20/250 | KLAL | 12 | 20/30 | Complete | Mycophenolate mofetil + tacrolimus | Phaco, IOL | ||
| 12 | 8 | 50 | F | OD | 12 (Total) | 20/100 | KLAL | 12 | 20/30 | Complete | Mycophenolate mofetil + tacrolimus | Phaco, IOL | ||
| 13 | 9 | 48 | F | OD | 10 (Superior) | Restasis, doxycycline | 20/60 | KLAL | 33 | 20/150 | Partial a | Tacrolimus | Phaco, IOL | |
| 14 | 9 | 48 | F | OS | 8 (Superior) | Restasis, doxycycline | 20/40 | KLAL | 41 | 20/50 | Partial a | Tacrolimus | Phaco, IOL |
a Partial resolution of symptoms owing to patient’s severe rosacea-related blepharokeratoconjunctivitis and meibomian gland dysfunction.
The mean duration of contact lens (CL) wear was 15.8 ± 6.9 years (range 1–20 years), and 79% of eyes (11/14) had between 15 and 20 years of CL use. All patients wore CLs for the correction of refractive error and reported daily usage of 10 or more hours. All eyes had symptoms of at least 1 of the following: photophobia (9/14), redness (4/14), tearing (3/14), pain (2/14), or foreign body sensation (1/14). On average, 10.4 ± 2.5 clock hours (range, 6–12 clock hours) of the limbus were affected.
Conservative treatments were attempted in all patients consisting of discontinuation of CL, frequent preservative-free artificial tears, vitamin A ointment before bed, topical steroids 4 times daily, oral doxycycline 100 mg, and topical cyclosporine 0.05% twice daily, alone or in combination for at least 3 months.
All patients had decreased BCVA at presentation, on average to 20/60 (range 20/30–20/250). Findings leading to a diagnosis of severe limbal stem cell deficiency included at least 6 clock hours of whorl-like epitheliopathy, an opaque epithelium arising from the limbus, late fluorescein staining of the involved epithelium, and superficial neovascularization or conjunctivalization. Complete conjunctivalization of the corneal surface was present in 64% of eyes (9/14). Bilateral severe limbal stem cell deficiency was present in 56% of patients (5/9). Conservative measures failed in all eyes.
Average time from date of diagnosis to date of surgery was 9.8 months (range 1–32 months). Average preoperative visual acuity was 20/70 (range, 20/40–20/250). A total of 71% of eyes (10/14) underwent keratolimbal allograft and 29% (4/14) underwent living-related conjunctival limbal allograft surgery. After an average follow-up of 26 months (range 12–70 months) after transplantation, 86% of eyes (12/14 eyes) had total symptom resolution, a BCVA of 20/30 or better, and a stable ocular surface. The improvement in BCVA after limbal stem cell transplantation was statistically significant ( P < .01).
Two eyes from 1 patient with severe rosacea blepharokeratoconjunctivitis had an improved ocular surface. No vision improvement, from baseline 20/150 OD and 20/60 OS, was evident in this patient at last follow-up. No eyes required subsequent penetrating keratoplasty.
With regard to patient systemic immunosuppression regimens, the average duration on prednisone use was 7.3 months (range 1.4–17 months). All patients were successfully tapered off of prednisone. At last follow-up, 5 of 9 patients and 2 of 9 patients, had successfully tapered off of tacrolimus and mycophenolate mofetil, respectively. The average duration of tacrolimus use before discontinuation was 24 months (range 16–34 months). The average duration on mycophenolate mofetil use before discontinuation was 24 months (range 23–25 months). Including patients still on immunosuppression at last follow-up, average duration on tacrolimus was 21 months (range 12–34 months) and on mycophenolate mofetil was 23 months (range 12–41 months).
Adverse events included nausea in 1 patient 1 month after surgery, which resolved with over-the-counter antiemetics; increased bilirubin levels in 1 patient 1 week after surgery, which normalized after cessation of Bactrim prophylaxis; and neutropenia in 1 patient 8 months after surgery, which resolved after cessation of Bactrim prophylaxis and treatment with granulocyte colony-stimulating factor (G-CSF). Fifty-seven percent of eyes (8/14) experienced elevated IOP requiring topical antiglaucoma treatment. Seventy-one percent of eyes (10/14) underwent subsequent cataract extraction. No episodes of rejection were noted during follow-up. Pain, sectoral conjunctival injection, edema, and local epithelial abnormality leading to an epithelial defect were considered signs of allograft rejection.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


