Purpose
To determine the lifetime risk and duration of blindness in patients with manifest open-angle glaucoma (OAG).
Design
Retrospective chart review.
Methods
We studied glaucoma patients who died between January 2006 and June 2010. Most glaucoma patients living in the catchment area (city of Malmö; n = 305 000) are managed at the Department of Ophthalmology at Skåne University Hospital in Malmö. From the patient records we extracted visual field status, visual acuity, and low vision or blindness as defined by the World Health Organization (WHO) criteria and caused by glaucoma at the time of diagnosis and during follow-up. We also noted age at diagnosis and death and when low vision or blindness occurred.
Results
Five hundred and ninety-two patients were included. At the time of the last visit 250 patients (42.2%) had at least 1 blind eye because of glaucoma, while 97 patients (16.4%) were bilaterally blind, and 12 patients (0.5%) had low vision. Median time with a glaucoma diagnosis was 12 years (<1-29), median age when developing bilateral blindness was 86 years, and median duration of bilateral blindness was 2 years (<1-13). The cumulative incidences of blindness in at least 1 eye and bilateral blindness from glaucoma were 26.5% and 5.5%, respectively, after 10 years, and 38.1% and 13.5% at 20 years.
Conclusions
Approximately 1 out of 6 glaucoma patients was bilaterally blind from glaucoma at the last visit. Median duration of bilateral blindness was 2 years.
The risk of visual disability from glaucoma is probably the most important question for a newly diagnosed glaucoma patient. It is well known that open-angle glaucoma (OAG) is a major reason for blindness, and that glaucoma is the second most important reason for blindness worldwide. Nevertheless, the risk of blindness attributable to glaucoma for a white patient with OAG is often assumed to be small. Several studies have addressed the risk of glaucoma blindness, but only few published studies followed glaucoma patients until death.
The average duration with a glaucoma diagnosis has been estimated to be approximately 13 years in white patients, but little is known about the duration of blindness in glaucoma patients.
We have access to data on a large and representative part of all diagnosed glaucoma patients in our catchment area (population 305 000). This gave us the opportunity to study the lifetime risk of low vision and blindness in patients with open-angle glaucoma as well as the time with visual impairment from glaucoma.
Methods
This retrospective study was conducted following the tenets of the Declaration of Helsinki. The Regional Ethical Review Board of Lund, Sweden approved the retrospective chart review and usage of the acquired data.
Approximately three-quarters of all known glaucoma patients in Malmö are diagnosed and followed at Skåne University Hospital, Malmö. Patients with permanent visual disability are referred to 1 institution: the Habilitation and Assistive Technology Service in Malmö. We used the patient administrative systems of both the hospital and the Habilitation and Assistive Technology Service in Malmö to identify patients with manifest glaucoma with visual field loss. Patients who died between January 1, 2006 and June 30, 2010 (according to the national tax registration system) were then included. The records of all identified patients were reviewed and all relevant data were noted.
Eligible patients had to have OAG, primary open-angle glaucoma (POAG), or exfoliative glaucoma (PEXG). Patients with other types of glaucoma were not included. Records of visual acuity (VA) and/or visual field (VF) examination during the last 3 years before patients’ deaths were required. Patients who were blind at the time of the last visit were included even if the time between the last visit and death exceeded 3 years.
Patients included in the study were divided into 2 groups: the first group included patients who had been followed at Skåne University Hospital already from the start, giving us access to visual acuity, visual field status, and age at the time of diagnosis. Patients in the other group were initially diagnosed outside Skåne University Hospital and referred to our outpatient department only later during follow-up. Complete data (including visual acuity and visual field status) for these patients were available from the first examination at the hospital. Here, we refer to the groups as the Data at Diagnosis and the Follow-up Only group, respectively.
For each included patient we recorded sex, age at death, and time between last visit and death. For patients in the Data at Diagnosis group (423/592, 71.5%) we also noted type of glaucoma (POAG or PEXG), age at diagnosis, and years with a glaucoma diagnosis. The presence of exfoliation syndrome (PEX) was recorded if noted at the time of diagnosis or up to 1 year later. In addition, all available data were reviewed to clarify if PEX had been documented in eyes that had undergone cataract surgery before the glaucoma diagnosis was established.
A diagnosis of glaucoma required that at least 1 eye: (1) showed a repeatable visual field defect (VFD) consistent with glaucoma and not explained by other causes; or (2) had only 1 visual field test but with a VFD consistent with glaucoma and a corresponding optic disc abnormality; or (3) was already blind (visual acuity <0.05) at time of diagnosis and had a record of a totally cupped glaucomatous optic disc.
Patients were excluded if other disease made it impossible to establish a glaucoma diagnosis with certainty or to determine whether the visual field showed glaucomatous field loss or not (eg, patients with optic disc drusen or endocrine ophthalmopathy).
Patients were routinely followed with standard automated perimetry using the Humphrey perimeter (Carl Zeiss Meditec, Dublin, California, USA) 30-2 or 24-2 Full-Threshold or SITA programs. Visual field defects were defined as glaucomatous if they showed a pattern consistent with glaucoma (eg, a nasal step or a paracentral or arcuate defect). In addition, the Glaucoma Hemifield Test (GHT) had to be classified as “borderline” or “outside normal limits.” Visual fields were considered reliable if false-positive responses were fewer than 15% and a clear blind spot could be seen in the visual field printouts (threshold value <10 dB). Nonglaucomatous fellow eyes without VF measurements at diagnosis were set to a mean deviation (MD) value of 0 dB, indicating a normal visual field.
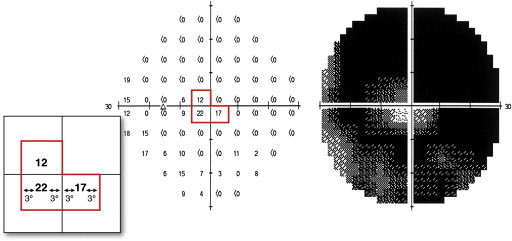
We registered best-corrected VA and the remaining visual field by measuring the widest diameter of the central visual field at the time of diagnosis or up to 1 year after diagnosis (in the Data at Diagnosis group only) and at the last visit before death (in all included patients). We used the recommendations of the United States Social Security Administration : a pseudoisopter was drawn by hand midway between points with threshold sensitivity values ≥10 dB and those with values <10 dB on the Humphrey Field Analyzer numerical dB printout ( Figure 1 ). The mean value was used if 2 threshold values were measured at a given test point location. This pseudoisopter was used to measure the widest diameter of the remaining central visual field, to assess if an eye was blind or had low vision.
Using the World Health Organization (WHO) criteria for low vision (0.05 [20/400] ≤ VA < 0.3 [20/60] and/or 10 degrees ≤ central VF < 20 degrees) and blindness (VA <0.05 [20/400] and/or central VF <10 degrees), we defined the following 4 categories of low vision and blindness with glaucoma as the main cause: (1) unilateral low vision: patients with low vision in 1 eye; (2) bilateral low vision: patients with low vision in the best eye; (3) unilateral blindness: patients blind in 1 eye; (4) bilateral blindness: patients with both eyes blind, mainly caused by glaucoma in at least 1 eye.
The cause of visual disability was determined by reviewing patient charts and analyzing the information in relation to the VF appearance. In most patients the main reason for visual disability was clear. In a few eyes it was impossible to determine a single cause of visual disability. Then we recorded a combination of causes.
The date of the glaucoma diagnosis was set to the date of the first reliable VF showing a glaucomatous defect. The time for low vision or blindness was the first visit when the Humphrey field was centrally constricted to less than 20 degrees or 10 degrees, respectively, or when VA was permanently reduced to below 0.3 (20/60) or 0.05 (20/400), respectively. Even in those few patients who had missed many consecutive visits during follow-up, all available data on visual function were analyzed as of the date from the next visit.
Statistical Analyses
Time with glaucoma blindness and the final outcomes in terms of low vision and blindness from glaucoma were determined in all included patients.
Cumulative incidence of blindness and time with diagnosed glaucoma were calculated in the Data at Diagnosis group. We chose to calculate cumulative incidences with a competing risk method. Contrary to the Kaplan-Meier method, the competing risk method does not “censor” individuals with competing risks. Thus, the probability of an event-free survival calculated with the competing risk method is a conditional probability, which takes both the event and the competing risks into account. In our analysis, blindness attributable to reasons other than glaucoma or death without blindness were modeled as competing risk events. Annual incidence rates were calculated setting all “study” events (blindness attributable to glaucoma) and all competing events to the time point just prior to the end of the annual period. In addition, cumulative incidences for blindness in at least 1 eye and bilateral blindness were calculated with the Kaplan-Meier method in order to be able to compare our results with previously published results.
The Pearson χ 2 test was used to compare the rates of low vision and blindness in the Data at Diagnosis and Follow-up Only groups. All statistical calculations were performed with SPSS version 19.0 (SPSS Inc, Chicago, Illinois, USA). Statistical significance was set to P < .05.
Results
Five hundred and ninety-two of 662 patients (89.4%) with manifest glaucoma with visual field loss met the inclusion criteria ( Figure 2 ). Three hundred and sixty-seven (62.0%) were female and 372 patients (62.8%) had glaucoma in both eyes. Seventeen of all included patients (2.9%) were registered in the administration system of the Habilitation and Assistive Technology Service only. Median time between last visit and death was 8 months (interquartile range 3-16 months). Median age at death was 87 years (range 50-103 years).
There were 423 patients in the Data at Diagnosis group (71.5%). In those patients mean age at diagnosis was 74.0 ± 7.9 years, ranging from 46-95 years. Exfoliative glaucoma was found in at least 1 eye in 170 patients (40.2%). Average perimetric MD at diagnosis was −5.59 ± 5.69 dB and −11.83 ± 8.18 dB in the better and the worse eye, respectively. Median VA at time of diagnosis was 0.8 (20/25), ranging from no light perception to 1.00 (20/20), in the perimetrically better eye and 0.8 (20/25), ranging from no light perception to 1.25 (20/16), in the perimetrically worse eye. Untreated mean intraocular pressure (IOP) value in all glaucomatous eyes at time of diagnosis was 27.2 ± 8.8 mm Hg.
Numbers of patients with low vision and blindness from glaucoma at the last visit are shown in the Table . At the last visit, 42.2% (250 of 592 patients) of all patients were blind from glaucoma in at least 1 eye and 16.4% in both eyes. Other reasons for unilateral blindness were age-related macular degeneration (AMD) (26 patients), a combination of cataract and other disease (10 patients), and other causes (32 patients). Seventeen patients were bilaterally blind because of reasons other than glaucoma (16 from AMD, 1 patient from other reason). A combination of causes for blindness was found in 1 eye of 7 blind patients ( Table ). There was no statistically significant difference in the frequencies of visual impairment at the last visit when comparing the Data at Diagnosis group and the Follow-up Only group ( Table , P = .260). In patients who developed blindness attributable to glaucoma, the median time with bilateral blindness was 2 years (<1-13) (mean 3.0 ± 3.1). Patients who became bilaterally blind from glaucoma did so at a median age of 86 years (range 66-98; mean 85.7 ± 6.1). Only 13 patients (13.5% of blind patients and 2.2% of all patients) became blind before the age of 80 years.
| All Patients (n = 592) n (%) | Follow-up Only Group (n = 169) n (%) | Data at Diagnosis Group (n = 423) n (%) | |
|---|---|---|---|
| Unilateral low vision | |||
| OAG | 52 (8.8) | 13 (7.7) | 39 (9.2) |
| Bilateral low vision | |||
| OAG + OAG | 7 (1.2) | 2 (1.2) | 5 (1.2) |
| OAG + other cause | 5 (0.9) | 1 (0.6) | 4 (0.9) |
| In total: | 12 (2.0) | 3 (1.8) | 9 (2.1) |
| Unilateral blindness | |||
| OAG | 153 (25.8) | 51 (30.2) | 102 (24.1) |
| Bilateral blindness | |||
| OAG + OAG | 67 (11.3) | 22 (13.0) | 45 (10.6) |
| OAG + other cause | 30 (5.1) | 10 a (5.9) | 20 b (4.7) |
| In total | 97 (16.4) | 32 (18.9) | 65 (15.4) |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


