5
Lifestyle Changes for Tinnitus Self-Management
We agree with Duckro et al (1984, p. 460), who wrote: “As with chronic pain, the treatment of chronic tinnitus is more accurately described in terms of management rather than cure.” The goal of tinnitus management is to reduce the severity of tinnitus until it is no longer a negative factor in the patient’s life. Appropriate lifestyle changes can facilitate this process.
To recommend specific lifestyle changes that will help tinnitus patients to improve their overall condition, an effective tinnitus management program should include the following:
• Clinicians who are willing to spend a substantial amount of time (up to several hours) with each patient
• Analysis of detailed health and psychosocial profiles of patients
• An interview/education session
• When possible, inclusion of spouses, significant others, relatives, or friends in the evaluation and treatment processes
Before recommendations for lifestyle changes can be formulated, factors contributing to tinnitus severity must be identified for each patient. We mail detailed questionnaires to patients prior to their initial tinnitus clinic appointment. Three of the questionnaires request information about patients’ health, hearing, and tinnitus histories (see Johnson, 1998, for questionnaire format and content). Twelve of the questions constitute a Tinnitus Severity Index (Meikle et al, 1995; see Fig. 5–1) that assesses the negative impacts of tinnitus on patients. Patients also fill out the State-Trait Anxiety Inventory (STAI; Spielberger, 1998) and an abbreviated version of the Beck Depression Inventory (Beck and Beck, 1972).
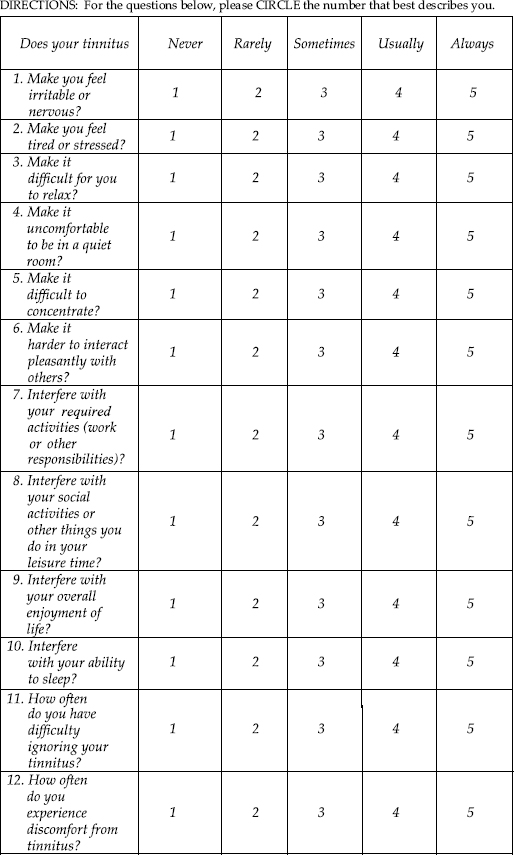
Figure 5–1 Tinnitus Severity Index questions.
After reviewing the patient’s medical records and responses to questionnaires, we spend 1 to l½ hours interviewing each patient. This interview session serves several important purposes:
• It gives patients the opportunity to clarify and elaborate on their questionnaire responses.
• It gives clinicians the opportunity to ask additional questions.
• If patients are accompanied by spouses, friends, or relatives, these companions often provide important details about the patient’s physical and emotional state, social and work history, communication difficulties, and so on.
• During the interview, clinicians identify specific problem areas and discuss them with the patient.
• When possible, clinicians suggest strategies, protocols, or devices that are likely to reduce the severity of the patient’s tinnitus. Diagnostic testing is sometimes required before specific tinnitus management strategies are suggested.
• Part of the interview session is spent educating patients about possible causes of their tinnitus as well as reassuring and counseling them regarding factors that could exacerbate or improve their condition. If patients understand that their tinnitus is nothing more dangerous than a perception of sound, they will be able to pay less attention to it.
Recommended Lifestyle Changes
Adjust Patient Expectations and Perspective
Before patients arrive for their appointment in our clinic, we inform them in writing that we cannot “cure” their tinnitus. We also remind patients of this fact during their initial interview. Adjusting patient expectations into the reasonable range is an important step in the process of reducing tinnitus severity. However, as Tyler et al (2001) suggested, it is also important to provide patients with hope. Even though a cure for most cases of chronic tinnitus is not available now, there are many ways for patients to obtain relief from the symptoms.
The following observations have been made about patients who suffer from severe tinnitus: they tend to be very somatically aware and internally directed (i.e., they are high self-attenders; Newman et al, 1997); they often resent the persistence of the noises, wish to escape them, and worry excessively about their health and sanity (Hallam et al, 1988); and they have maladaptive coping strategies (this includes patients who attempt to avoid tinnitus, pray that their tinnitus will go away, and fantasize about not having tinnitus). Maladaptive coping strategies also include dwelling on tinnitus, talking to others about how unpleasant the noises are, and catastrophizing about the consequences of tinnitus (Budd & Pugh, 1996). Catastrophic thinking is reflected in statements by patients such as “My entire life has been disrupted and it is a daily struggle…. There is never any peace or escape” (Neher, 1991) A study by Budd and Pugh (1995) demonstrated that patients who believe tinnitus is beyond their control (“externals”) are more likely to experience severe tinnitus, anxiety, and depression than patients who believe they can exert some control over their symptoms and other life events (“internals”).
House (1981) made the following observations:
• Tinnitus as a symptom can become a scapegoat.
• Conflicts and needs are displaced on this symptom—it can be a chief concern and often an obsession.
• This obsession leads to other neurotic behavior, such as social withdrawal, isolation, and difficulty with reality contact.
• In some cases the tinnitus seems to take on the role of secondary gain—it can relieve the guilt associated with job failure or social conflicts.
It is important for patients to recognize that not all of their problems are necessarily attributable to tinnitus. Patients should be encouraged to identify problems that can be treated apart from their tinnitus. For example, some patients blame tinnitus for difficulties that are actually caused by hearing loss (e.g., difficulty understanding speech in noisy environments). Amplification will improve speech perception for many of these patients and can also reduce the loudness of their tinnitus.
Identification and treatment of problems mistakenly or disproportionately attributed to tinnitus can result in a reduction of importance patients assign to tinnitus. This will ultimately facilitate a reduction of tinnitus severity.
Rizzardo et al (1998, p. 24) stated that there appears to be a “link between psychological distress and tinnitus in a potential somatopsychological and psychosomatic vicious [cycle] (a psychological predisposition to react emotionally to events, tinnitus as a source of distress that reinforces the symptom, accentuating hypochondriac fears).”
Because patients with severe tinnitus sometimes develop cognitive distortions, including catastrophic thinking, cognitive-behavioral therapy can be useful (Andersson et al, 2001; Wayner, 1998). Some patients who exhibit maladaptive coping strategies improve when they are provided with cognitive coping strategies that are designed to help them interpret stressful situations and their disorder in more positive, adaptive ways (Holroyd et al, 1977; Kirsch et al, 1989).
Clinicians should strive to improve patients’ understanding of tinnitus and their perspective about the symptom, and provide strategies for coping with tinnitus during the education and counseling portions of appointments. However, a series of ongoing psychotherapy sessions is sometimes necessary for patients to make significant improvements in these areas. When appropriate, clinicians should encourage patients to pursue psychological counseling. Also, when possible, clinicians should provide referrals to mental health professionals who practice near the patient’s home.
Improve Sleep Patterns
Patients who experience insomnia also tend to experience more severe tinnitus than patients who do not have trouble sleeping (Folmer and Griest, 2000). Improvements in sleep patterns are often associated with reductions in tinnitus severity (Folmer, 2002). If patients are not sleeping long enough or restfully enough, clinicians can recommend the following:
• Patients can bring pleasant sounds into the bedroom to reduce their perception of tinnitus. Of help are pillows embedded with flat speakers that can be connected to any sound source. Tabletop sound generation machines also are useful. These machines play various soothing sounds, such as raindrops and ocean waves, and have an input jack for speaker pillows.
• If necessary, patients could use an over-the-counter sleep medication such as Alluna, Sominex, melatonin, Tylenol P.M., or Benadryl.
• If necessary, patients should talk to their physician about using prescription sleep medication such as Ambien or trazodone. Sleep medications should be used as needed, not necessarily every night. After sleep patterns stabilize, patients should try to reduce their usage of sleep medications.
• Patients should consult the list of recommendations provided by the National Sleep Foundation (www.sleepfoundation.org).
• Patients should pursue activities and develop strategies that promote stress reduction and relaxation. Relaxation/stress management therapy may be warranted.
• If insomnia persists, patients should go to a specialized sleep clinic for evaluation and treatment.
If patients report that they usually get enough restful sleep yet still feel tired while they are awake, clinicians should recommend that they have a complete physical examination, including blood tests of thyroid function (thyroxine or thyroid-stimulating hormone levels) and hemoglobin concentration. Successful treatment of hypothyroidism or anemia often relieves fatigue experienced by patients who have these disorders.
Reduce Anxiety
Tinnitus severity is positively correlated with patients’ level of anxiety (Folmer et al, 2001). Therefore, stress reduction is imperative for anxious patients. We use the State-Trait Anxiety Inventory (STAI) (Spielberger, 1998) to assess anxiety levels in our tinnitus patients. The average State Anxiety score (20 questions; minimum score 20, maximum score 80) for working adults is 35.5 ± 10.5 (Spielberger et al, 1983). If a patient scores 46 or higher on the questionnaire, anxiety management strategies should be recommended.
Like many psychological co-symptoms, anxiety is associated with other factors such as insomnia, depression, communication difficulties, and employment, financial, or social problems. For patients who exhibit anxiety disorders, we recommend evaluation by a psychiatrist, preferably one who specializes in stress management. Other patients may benefit from stress reduction or relaxation techniques taught by licensed therapists or counselors. The Anxiety Disorders Association of America (Silver Spring, MD; www.adaa.org) can help patients locate a qualified therapist.
Some patients benefit from hypnosis; some benefit from biofeedback; others benefit from an exercise program, yoga, meditation, or regular massage. Almost anything that reduces the patient’s level of stress or anxiety will decrease the severity of the tinnitus and will also help the person relax and sleep. Anxiolytic medication is necessary for some patients with severe anxiety.
Evaluation and Treatment of Depressed Patients
Depressed patients perceive their tinnitus to be more severe than do nondepressed patients (Folmer et al, 1999). In fact, the severity of tinnitus is positively correlated with the severity of patients’ depression (Folmer et al, 2001). Identification and treatment of depression are essential elements of an effective tinnitus management program. The U.S. Preventative Services Task Force (2002) recommended screening adult patients for depression. In its simplest form, this screening can be accomplished by asking patients two questions, such as, During the past 2 weeks, have you felt down, depressed, or hopeless? and During the past 2 weeks, have you felt little interest or pleasure in doing things? Affirmative responses to these questions should be followed by a more comprehensive analysis of depressive symptoms.
We use an abbreviated version of the Beck Depression Inventory (aBDI)—consisting of 13 multiple-choice questions—to assess depression in tinnitus patients (Beck and Beck, 1972). A score between 5 and 7 on the aBDI indicates mild depression. A score between 8 and 15 indicates moderate depression; a score of 16 or more indicates severe depression. The aBDI is a useful instrument because it is easy to administer and can identify depression in patients who do not recognize or admit the severity of their own depression. If a patient scores 8 or more on the aBDI, we recommend that he or she receives effective treatment for depression. If the patient has not yet received any treatment for depression, we first recommend evaluation by a psychiatrist. This should be followed by an ongoing series of psychotherapy sessions and possibly antidepressant medication.
Folmer (2002) analyzed the association between aBDI scores and Tinnitus Severity Index scores for 190 patients 6 to 36 months after their initial appointment in a tinnitus clinic. Patients whose Beck Depression score decreased 3 or more points at follow-up exhibited significant reductions in Tinnitus Severity Index scores. Patients whose follow-up Beck Depression score stayed within 0 to 2 points of their initial Beck score exhibited a smaller degree of improvement in tinnitus severity. However, patients whose initial Beck Depression score increased 3 or more points on the follow-up questionnaire did not exhibit significant changes in Tinnitus Severity Index scores. These results illustrate the importance of effective treatment for depression when it is present in tinnitus patients.
Break the Vicious Cycle
As illustrated in Fig. 5–2, the symptoms of tinnitus, fatigue, anxiety, and depression can form a vicious cycle and exacerbate each other (Folmer et al, 2001). Tinnitus is not always the starting point of this cycle. The cycle can begin at any point and progress in any direction. Some patients experienced depression, insomnia, or anxiety before their tinnitus began. A combination of medication and/or psychotherapy will typically reduce the severity of these symptoms and associated tinnitus. Patients should be encouraged to show Fig. 5–2 to psychiatrists or psychologists during their initial session with these clinicians. The diagram will help clinicians to understand the relationships among these symptoms associated with severe tinnitus. Specific tinnitus expertise is not required of mental health professionals in order for them to help patients. If clinicians can facilitate reductions in patients’ levels of insomnia, anxiety, and depression, the severity of tinnitus should also decrease (Folmer, 2002).
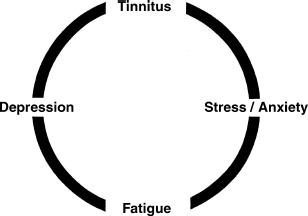
Figure 5–2 A vicious cycle of symptoms.
Address Communication Problems
Approximately 90% of all tinnitus patients have some degree of hearing loss (Meikle, 1997). Many of these patients report significant problems understanding conversations, television programs, movies, and so on. For patients who may benefit from amplification, we recommend a trial period with appropriate hearing aids. We also give information to patients regarding assistive listening devices and effective communication strategies.
Utilize Acoustic Therapy
Most patients report that tinnitus is more noticeable in quiet environments, such as their home at night. Clinicians should give this recommendation to every patient: add pleasant sounds to any environment that is too quiet. Regardless of which devices are used, the rationale for acoustic therapy remains the same: increase the level of external sounds in the patient’s environment to decrease the patient’s perception of tinnitus. Acoustic therapy devices include hearing aids, in-the-ear sound generators, in-the-ear combination instruments (hearing aid plus sound generator), tabletop sound machines, sound pillows, pillow speakers, audiotapes or compact discs, and fans.
Evaluate and Modify Medications
No medications are particularly effective for reducing the severity of tinnitus (Dobie, 1999). When appropriate, clinicians should recommend that patients consult with their physician about prescription medications to treat insomnia, anxiety, depression, phobias, obsessive-compulsive tendencies, or other psychological problems. For complex problems such as anxiety disorders or major depression, medication alone is seldom the answer. In fact, we place more importance on psychotherapy than medications in the treatment of these conditions. Patients may benefit from occasional, short-term use of anxiolytic or hypnotic medications. Some patients also benefit from using antidepressant medications. However, patients will not necessarily need to use any of these medications for the rest of their lives. Clinicians should give all patients the goal of eventually improving to the point where they no longer need to take such medications. In some cases, effective psychotherapy can help patients progress so that prescription medications for sleep, anxiety, or depression are no longer required.
Anything that affects a patient’s metabolism can affect his or her hearing or tinnitus. For this reason, medical conditions such as hyper- or hypothyroidism, hyper- or hypoglycemia, hyperlipidemia, and hypertension must be identified and treated with appropriate medications as indicated.
Some patients take potentially ototoxic medications without knowing it. For example, patients take quinine-based medications for a variety of conditions, including leg cramps or restless legs. Patients with a history of epileptic activity sometimes take the antiseizure medication valproic acid. Some patients have taken furosemide (Lasix) for years as a diuretic to control hypertension. These medications may or may not exacerbate hearing loss or tinnitus for a particular patient. However, because the Physicians’ Desk Reference (2005) lists hearing loss and tinnitus as common side effects of quinine, valproic acid, and furosemide, we recommend that patients talk to their physician about the possibility of switching to an alternative medication that does not have the same ototoxic potential.
Conversely, it is important that clinicians do not discourage patients from trying a medication just because the Physicians’ Desk Reference (2005) lists tinnitus as one of its potential side effects. Almost every antidepressant, anxiolytic or hypnotic medication has the potential to trigger tinnitus for a small percentage of people who take it. In the vast majority of cases, tinnitus resolves after the patient stops taking the medication. For patients who already experience chronic tinnitus, this should not be a reason for them to avoid medications that could benefit them. For example, patients with a history of cardiovascular or cerebrovascular disease should not avoid taking 81 mg of aspirin daily if it is recommended by their physician. This small amount of aspirin is unlikely to increase the loudness of their tinnitus (see Fig. 5–3). However, the anticoagulant and anti-inflammatory properties of aspirin could save their lives. Even if a patient’s tinnitus increases after taking a particular medication, the tinnitus should return to its normal level after the person stops taking the medication.
Some tinnitus patients have a long list of medications they are currently taking. If the medications being taken by a patient seem excessive, redundant, or potentially hazardous, we recommend that each of the prescribing physicians reviews the entire regimen and decides if the present combination and dosage of medications are appropriate.
Dietary Considerations
Most patients report that low to moderate consumption of caffeine does not affect their tinnitus. We do not recommend a moratorium on caffeine for these patients. They may continue to enjoy coffee, tea, caffeinated soft drinks, or chocolate. As shown in Fig. 5–3, only ∼9% of our patients report that caffeine increases the loudness of their tinnitus. In most of these cases, relatively high levels of caffeine consumption are responsible for increases in tinnitus. Instead, we recommend that patients reduce their intake of caffeine by switching to decaffeinated beverages as needed.
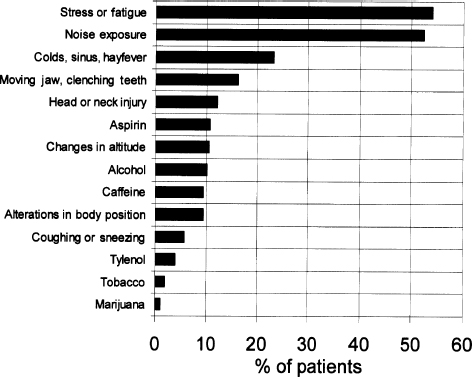
Figure 5–3 Factors that can increase tinnitus loudness (as reported by Oregon Health & Sciences University (OHSU) Tinnitus Clinic patients).
We make few other dietary recommendations for tinnitus patients. A small percentage of patients report that consumption of sugar, salt, dairy products, or other particular foods can increase the loudness of their tinnitus. As a result, patients voluntarily restrict their intake of these foods. Because such food sensitivity is relatively rare in the tinnitus patient population, clinicians should make dietary recommendations on an individual basis. Most patients are free to enjoy a varied, sensible diet.
ALCOHOL
Low to moderate consumption of alcohol is not a problem for most patients (see Fig. 5–3). In fact, many patients report that a drink or two helps them to relax and to be less bothered by tinnitus. Usually a greater volume of alcohol is required to increase tinnitus. A rule of thumb: when a person has consumed enough alcohol to initiate hangover symptoms (including headache), this seems to be the amount of alcohol that will also increase tinnitus. If a person consumes this much alcohol on a regular basis, it is probably excessive, and the patient should be evaluated for alcoholism. Using alcohol as a sleep aid is not recommended because metabolites of alcohol often interrupt sleep a few hours after drinking.
DIETARY SUPPLEMENTS
There are no dietary supplements or herbal or homeopathic preparations that are particularly effective at reducing the severity of tinnitus. In a double-blind placebo-controlled study of 1121 tinnitus patients, Drew and Davies (2001) reported that Ginkgo biloba was not more effective than placebo at reducing the severity of tinnitus. Therefore, we do not recommend this supplement for tinnitus relief.
Most patients should take a multivitamin/mineral supplement daily after eating. These supplements alone will probably not reduce the loudness or severity of a patient’s tinnitus. However, they should help to maintain or improve the patient’s general health, including the integrity and functioning of the auditory system. Taking appropriate dietary supplements can also improve a patient’s sense of well-being. Patients who take an active role in their own health maintenance feel that they have greater control over their condition. This positive perspective can contribute to increased optimism and ultimately to reductions in tinnitus severity.
Exercise
Some patients reduce their level of physical activity because exercising increases the loudness of their tinnitus. This increase in tinnitus is almost always temporary and is related to increased blood pressure during exertion. Because the benefits of regular exercise (including stress reduction, improved cardiovascular health, muscle tone, mood, and sleep patterns) far outweigh a temporary increase in tinnitus, we recommend that patients engage in a variety of physical activities when possible.
Reduce Unprotected Noise Exposure
As shown in Fig. 5–3, more than 50% of our patients report that excessive noise exposure can increase the loudness of their tinnitus. We encourage patients to wear earplugs or earmuffs as protection against harmful sounds (gunfire, gas lawn mowers, leaf blowers, chain saws, circular saws, heavy machinery, loud music, etc.) because noise-induced hearing loss will compromise patients’ communication abilities and may also contribute to permanent increases in their tinnitus. Clinicians can educate patients about the mechanisms and permanent nature of noise-induced hearing loss by using large ear models and photomicrographs of hair cells damaged by excessive noise exposure (see e.g., Slepecky, 1986). Patients should be shown evidence of their own noise-induced hearing loss during discussions of the results of audiometric tests.
Desensitize the Patient’s Auditory System
Hypersensitivity to sound causes some patients to develop aversions to restaurants, movies, sporting events, concerts, parties, or church services and to abhor the sounds of a vacuum cleaner, sirens, bus brakes, or silverware striking plates or drinking glasses. Clinicians should explain to patients that their increased sensitivity to sounds is a reflection of damage to outer hair cells that results in a form of recruitment. There is a real physiological reason—damage to the auditory system—that some sounds bother patients more than they used to. However, some patients develop extreme phonophobia, and wear earplugs most of the time. These patients often withdraw from the workplace and all forms of socialization. Fear of sound exposure can cause them to become reclusive. This exaggerated response is a reflection of the patient’s mental state and coping skills. In these cases, we make the following recommendations:
• Patients should stop wearing hearing protection unless they are exposed to hazardous levels of sound. Overuse of earplugs or earmuffs can contribute to hypersensitization of the auditory system.
• To desensitize their auditory system, we encourage patients to listen to pleasant sounds (e.g., music or water/masking sounds) at comfortable levels. Patients can listen to these sounds through headphones, speakers, or inthe-ear sound generators. In addition to desensitizing patients’ auditory system, this may help to reduce patients’ fear of sounds.
• Patients should be encouraged to increase socialization, resume employment if they are able, and rejoin society as soon as possible. It is true that the urban environment is often noisy, but becoming a recluse because of phonophobia is not a healthy lifestyle.
• When appropriate, we recommend mental health evaluations and psychotherapy to help patients break their cycle of fearful thoughts and behaviors.
Modify Employment Status or Responsibilities
Most patients say their tinnitus is less bothersome when they are busy. Even if patients are retired or physically or mentally disabled, it is important for them to occupy their time with enjoyable and rewarding activities such as hobbies or volunteer work. They will then have less time to dwell or focus on their tinnitus. Patients should be encouraged to seek employment or to continue working if they are able to do so. Employment can provide patients with a sense of purpose, increased self-esteem, optimism, and financial stability. In addition to experiencing depression and having low self-esteem and few financial resources, unemployed patients often exaggerate the magnitude of their auditory symptoms. Patients who are too young to retire and are physically and mentally able to work should be encouraged to do so. Even a relatively simple part-time job is preferable to staying home every day and receiving a stipend from a governmental agency.
We give a copy of the Newsweek article “Healing Myself with the Power of Work” (Norlen, 1999) to patients who need encouragement to seek employment. The author of the article was an attorney who stopped practicing law after 6 years because of severe depression. A job he took delivering morning newspapers helped him to regain his self-esteem and perspective. He concluded, “One day soon I’ll be ready to leave this job behind, but I’ll never again view work as just a paycheck or a daily obligation. It will always be a part of my therapy, my healing. I don’t know where my next job will be, in the courtroom, the classroom or the office. But wherever it is, my work will be a weapon in my arsenal against the attacks I know will come again and again.”
Many of the observations in the article apply to tinnitus patients who have stopped working and socializing because of depression and despair. As it did for the article’s author, gainful employment can help tinnitus patients to feel more productive and hopeful. The article brings up another common theme: some people dislike their present job and feel stressed about going to it every day. Remember that House (1981, p. 198) observed that “tinnitus as a symptom can become a scapegoat… it can relieve the guilt associated with job failure or social conflicts.” Some patients use tinnitus as an excuse for quitting a job they don’t like because their work or workplace elicits unacceptable levels of stress for them. It is beneficial for such patients to realize that tinnitus is not the main problem at their workplace. Clinicians should help patients to make this distinction whenever possible. We do not usually encourage patients to quit their current job because such an action has financial and personal consequences that go beyond our clinical responsibilities. However, if it is clear that a patient does not want to continue in his or her current position, we help the patient to explore other possibilities. State vocational rehabilitation agencies can assist patients in this process.
Tinnitus and hearing loss can interfere with patients’ abilities to perform some jobs. Information about different types of hearing aids, effective communication strategies, and assistive listening devices such as telephone amplifiers or FM systems should be given to patients who complain about communication problems at work.
Patients in noisy professions must take precautions to protect their hearing. In some cases, tinnitus patients need to modify their work environment or duties to minimize occupational noise exposure. When necessary, patients should seek employment in a quieter environment within their current company or with a new employer.
Cultivate Personal Relationships/Increase Socialization
Personal relationships can suffer because of tinnitus or sound sensitivity. Some patients reduce socialization because of discomfort in noisy environments or because they are not sure how they may feel on a given occasion. Clinicians should encourage patients to continue employment and participation in social activities as much as possible for the following reasons:
• When patients are busy, their tinnitus is less noticeable and less bothersome.
• Social contact can help patients to achieve or maintain a healthy perspective about their auditory symptoms.
• If patients stop working and socializing, they often give in to counterproductive feelings of hopelessness and despair. They then attribute a disproportionate amount of importance to their auditory symptoms.
• Friends, family members, and coworkers are more likely to be sympathetic and lend support to the patient if the person gives realistic descriptions of the symptoms and makes efforts to persevere in spite of them.
• Patients feel better about themselves and more optimistic about the future if they remain active members of society.
Patients with supportive social and family relationships usually have more success coping with chronic medical conditions. Sullivan et al (1994) reported that patients who sought social support and those who had positive interactions with their spouse exhibited less tinnitus-related dysfunction than patients who did not experience supportive personal relationships.
Referrals to Other Health Care Professionals
If we detect any additional medical conditions that should receive evaluation or treatment, we refer patients to their primary care physician or to clinical specialists.
Conclusion
If patients can be motivated to implement positive lifestyle changes such as those described in this chapter, their overall condition will improve and the severity of their tinnitus will decrease. The key word in this process is implementation: patients need to make concrete efforts to follow specific recommendations formulated by health care professionals. Patients should be encouraged to take responsibility for their own improvement. Ultimately, the motivation to initiate and maintain positive lifestyle changes must come from within each patient.
References
Andersson G, Vretblad P, Larsen HC, Lyttkens L. Longitudinal follow-up of tinnitus complaints. Arch Otolaryngol Head Neck Surg 2001;127:175–179
Beck AT, Beck RW. Screening depressed patients in family practice: a rapid technic. Postgrad Med 1972;52(6):81–85
Budd RJ, Pugh R. The relationship between locus of control, tinnitus severity, and emotional distress in a group of tinnitus sufferers. J Psychosom Res 1995;39(8):1015–1018
Budd RJ, Pugh R. Tinnitus coping style and its relationship to tinnitus severity and emotional distress. J Psychosom Res 1996;41(4):327–335
Dobie RA. A review of randomized clinical trials in tinnitus. Laryngoscope 1999;109(8):1202–1211
Drew SJ, Davies WE. Effectiveness of Ginkgo biloba in treating tinnitus: double blind, placebo controlled trial. BMJ 2001;322(7278):1–6
Duckro PN, Pollard CA, Bray HD, Scheiter L. Comprehensive behavioral management of complex tinnitus: a case illustration. Biofeedback Self Regul 1984;9(4):459–469
Folmer RL. Long-term reductions in tinnitus severity. BMC Ear Nose and Throat Disorders 2002;2:3. Available at: www.biomedcentral.com/1472-6815/2/3
Folmer RL, Griest SE. Tinnitus and insomnia. Am J Otolaryngol 2000;21(5):287–293
Folmer RL, Griest SE, Martin WH. Chronic tinnitus as phantom auditory pain. Otolaryngol Head Neck Surg 2001;124(4):394–400
Folmer RL, Griest SE, Meikle MB, Martin WH. Tinnitus severity, loudness and depression. Otolaryngol Head Neck Surg 1999;121:48–51
Hallam RS, Jakes SC, Hinchcliffe R. Cognitive variables in tinnitus annoyance. Br J Clin Psychol 1988;27:213–222
Holroyd KA, Andrasik F, Westbrook T. Cognitive control of tension headache. Cog Ther Res 1977;1:121–133
House PR. Personality of the tinnitus patient. Ciba Found Symp 1981;85:193–203
House PR. Personality of the tinnitus patient. J Laryngol Otol 1984;98(Suppl 9):233
Johnson RM. The masking of tinnitus. In: Vernon JA, ed., Tinnitus Treatment and Relief. Boston: Allyn & Bacon; 1998:164–186
Kirsch CA, Blanchard EB, Parnes SM. Psychological characteristics of individuals high and low in their ability to cope with tinnitus. Psychosom Med 1989;51:209–217
Meikle MB. Electronic access to tinnitus data: the Oregon Tinnitus Data Archive. Otolaryngol Head Neck Surg 1997;117:698–700
Meikle MB, Griest SE, Stewart BJ, Press LS. Measuring the negative impact of tinnitus: a brief severity index. Abstr Assoc Res Otolaryngol 1995;167
Neher A. Tinnitus: the hidden epidemic, a patient’s perspective. Ann Otol Rhinol Laryngol 1991; 100:327–330
Newman CW, Wharton JA, Jacobson GP. Self-focused and somatic attention in patients with tinnitus. J Am Acad Audiol 1997;8:143–149
Norlen M. Healing myself with the power of work. Newsweek October 25,1999;12
Physicians’ Desk Reference. Montvale, NJ: Medical Economics; 2005
Rizzardo R, Savastano M, Bona Maron M, et al. Psychological distress in patients with tinnitus. J Otolaryngol 1998;27(1):21–25
Slepecky N. Overview of mechanical damage to the inner ear: noise as a tool to probe cochlear function. Hear Res 1986;22:307–321
Spielberger CD. State-Trait Anxiety Inventory for Adults (Form Y). Palo Alto, CA: Mind Garden; 1998
Spielberger CD, Gorsuch RL, Lushene R, Vagg PR, Jacobs GA. State-Trait Anxiety Inventory for Adults: Sampler Set, Manual, Test, Scoring Key. Palo Alto, CA: Mind Garden; 1983
Sullivan M, Katon W, Russo J, Dobie R, Sakai C. Coping and marital support as correlates of tinnitus disability. Gen Hosp Psychiatry 1994;16:259–266
Tyler R, Haskell G, Preece J, Bergan C. Nurturing patient expectations to enhance the treatment of tinnitus. Sem Hear 2001;22(1):15–21
U.S. Preventative Services Task Force. Screening for depression: recommendations and rationale. Ann Intern Med 2002;136:760–764
Wayner DS. Cognitive therapy and tinnitus: an intensive weekend workshop. In: Vernon JA, ed. Tinnitus Treatment and Relief. Boston: Allyn & Bacon; 1998:116–130
< div class='tao-gold-member'>



