Endoscopic surgery using an expanded endonasal approach now allows surgical access to an increasing range of parasellar, suprasellar, clivus, and petrous apex lesions. Accurate preoperative planning requires proper interpretation of CT and MRI results. It is essential to identify important anatomic landmarks and to recognize the appearance of common lesions and pseudolesions. Postoperative imaging must evaluate for residual tumors and identify iatrogenic conditions.
An expanded endonasal approach is being increasingly used not only for suprasellar and parasellar lesions but also for lesions of the clivus and medial petrous apex . As these endoscopic techniques advance, it becomes important for nonradiologists to understand the imaging anatomy of various skull base structures. Thin-section CT and MRI play a role in this area. Because the two modalities produce images based on different physical properties of tissue, they can often play a complementary role in localizing and characterizing lesions in the pre- and postoperative settings.
This article begins with a discussion of the parasellar and petrous apex radiologic anatomy, followed by a discussion of frequently encountered lesions in these regions. Also emphasized are nonpathologic entities that may mimic pathology radiographically (pseudolesions).
Parasellar structures
The cavernous sinus consists of bilateral structures containing multiple small venous sinusoids . Its floor rests on the intracranial surface of the sphenoid and temporal bones. A groove on the surface of the sphenoid bone is termed the carotid sulcus and marks the course of the horizontal segment of the intracavernous carotid. The medial wall of the cavernous sinus has a sellar portion (facing the pituitary and sella) and a sphenoidal portion (facing the body of the sphenoid). The lateral aspect of the sinus is separated from the middle cranial fossa by two layers of dura (meningeal and endosteal) reflected from the floor of the calvaria . By contrast, only a single thin layer of dura invests the medial wall. Anteriorly the cavernous sinus reaches the posterior border of the superior orbital fissure. Posteriorly the dural lining of the sinus merges with that of Meckel cave. Several schemes have been devised to define anatomic compartments within the sinus; almost all include medial and lateral components.
The cavernous sinus communicates with numerous skull base venous structures, most notably the superior and inferior petrosal sinuses, the basilar sinus, and the superior ophthalmic vein. Named portions of the intracavernous carotid artery are its posterior and anterior genus and the intervening horizontal segment. The artery lies in the medial compartment of the sinus, and in about half of cases directly abuts the medial wall.
The sinus is traversed by several nerves: the oculomotor (cranial nerve [CN] III), trochlear (CN IV), and abducens (CN VI) nerves, as well as the ophthalmic (CN V-1) and maxillary (CN V-2) branches of the trigeminal nerve. Microdissection shows that the oculomotor, trochlear, ophthalmic, and maxillary nerves (in order from superior to inferior) are associated with the inner dural layer at the lateral wall of the sinus ( Fig. 1 ) . The abducens nerve courses within the sinus (inferolateral to the horizontal segment of the cavernous carotid), but is still in the lateral compartment.
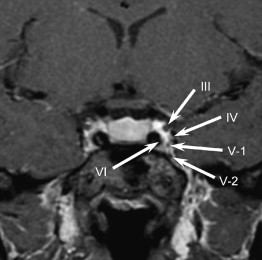
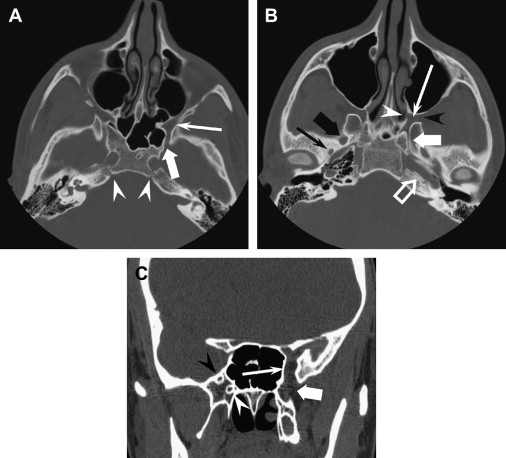
Anteriorly the oculomotor, trochlear, and abducens nerves, along with the ophthalmic branch of the trigeminal nerve, enter the orbit through the superior orbital fissure. The maxillary branch travels through the foramen rotundum to the pterygopalatine fossa ( Fig. 2 ). Multiple branches to the nasopharynx and alveolar ridge arise within the fossa, but the largest trunk continues as the infraorbital nerve to enter the orbit through the inferior orbital fissure. The pterygopalatine fossa also communicates medially with the nasal cavity through the sphenopalatine foramen, laterally with the masticator space through the pterygomaxillary fissure, and posteriorly with the middle cranial fossa by way of the Vidian canal. The Vidian canal is a pathway to the important landmark of the lacerum portion of the internal carotid artery .
Posteriorly the abducens nerve has a rather extended course through the basal cisterns before it enters the dura at the petroclival junction and inferior to the petroclinoid fold. At one time it was believed to travel along a constant fibro-osseous channel called the Dorello canal before entering the cavernous sinus. Recent microanatomic dissections show that it has a rather variable course through the petroclival venous confluence . The course of the nerve immediately posterior to the cavernous sinus is usually seen as a bilateral filling defect in the petroclival venous confluence on thin-section postcontrast images.
Slightly more superiorly and anteriorly the lateral dura of the cavernous sinus forms the Meckel cave, a large oval-shaped cerebrospinal fluid (CSF) pouch. The trigeminal ganglion lies within the Meckel cave and may enhance slightly. The mandibular branch of the trigeminal nerve does not enter the cavernous sinus, but descends through the foramen ovale. The ophthalmic and maxillary branches course along the inferior portion of the lateral wall of the cavernous sinus.
Petrous apex anatomy
The petrous portion is the most medial aspect of the temporal bone. It is bounded medially by the petro-occipital synchondrosis (see Fig. 2 ), which contains embryonic rests capable of becoming chondroid neoplasms. In sagittal plane, the petrous bone has a triangular shape with anterior wall forming the posterior margin of the middle cranial fossa and the posterior wall forming the anterior margin of the posterior cranial fossa. The tentorium attaches to the apex of the triangle, with the superior petrosal vein coursing near its attachment; in many patients there is a discernible bony groove for this vessel.
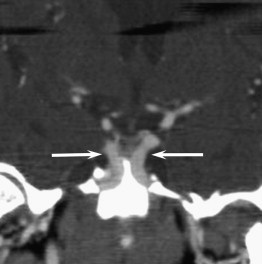
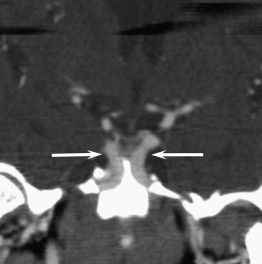
One of the most important surgical landmarks at the skull base is the course of the petrous and parasellar internal carotid arteries. The internal carotid artery enters the skull base just anterior to the jugular foramen and medial to the styloid process. The petrous canal then ascends vertically for about 1 cm before turning into horizontal plane at its first (lateral) genu. The horizontal segment of the petrous carotid continues anteromedially in the petrous bone. It turns vertically at its second genu and courses over the superior aspect of the cartilage-filled foramen lacerum. This lacerum segment is an important landmark for the expanded endonasal approach to the petrous apex. Ordinarily, the cavernous internal carotid arteries are symmetric in appearance and are separated by about 1.5 cm. A medial orientation (“kissing carotids”) is occasionally seen in either the cavernous or supraclinoidal carotids, however ( Fig. 3 ), which may be accompanied by thinning of the bony lateral wall of the sphenoid sinus leaving the vessel dehiscent into the sinus.
Petrous apex anatomy
The petrous portion is the most medial aspect of the temporal bone. It is bounded medially by the petro-occipital synchondrosis (see Fig. 2 ), which contains embryonic rests capable of becoming chondroid neoplasms. In sagittal plane, the petrous bone has a triangular shape with anterior wall forming the posterior margin of the middle cranial fossa and the posterior wall forming the anterior margin of the posterior cranial fossa. The tentorium attaches to the apex of the triangle, with the superior petrosal vein coursing near its attachment; in many patients there is a discernible bony groove for this vessel.
One of the most important surgical landmarks at the skull base is the course of the petrous and parasellar internal carotid arteries. The internal carotid artery enters the skull base just anterior to the jugular foramen and medial to the styloid process. The petrous canal then ascends vertically for about 1 cm before turning into horizontal plane at its first (lateral) genu. The horizontal segment of the petrous carotid continues anteromedially in the petrous bone. It turns vertically at its second genu and courses over the superior aspect of the cartilage-filled foramen lacerum. This lacerum segment is an important landmark for the expanded endonasal approach to the petrous apex. Ordinarily, the cavernous internal carotid arteries are symmetric in appearance and are separated by about 1.5 cm. A medial orientation (“kissing carotids”) is occasionally seen in either the cavernous or supraclinoidal carotids, however ( Fig. 3 ), which may be accompanied by thinning of the bony lateral wall of the sphenoid sinus leaving the vessel dehiscent into the sinus.
Imaging techniques
CT examination is best performed on a multislice scanner with axial images reconstructed at 1.25-mm or smaller intervals. Although direct coronal images were once performed, coronally oriented reformats are now technically excellent and minimize radiation dose to the patient. Both soft tissue and bone reconstructions should be performed; the latter can evaluate for subtle osseous erosion or remodeling.
Although MRI lacks the bony definition of CT, it is invaluable for demonstrating subtle soft tissue abnormalities on pre- and postcontrast imaging. The multiplanar capability aids in visualization of abnormalities in relation to anatomic landmarks. Diagnostic imaging studies usually include postcontrast images in at least axial and coronal planes. At least one plane should be imaged with fat saturation technique to better differentiate pathology from the intrinsically high T1 signal seen in normal fat in the cavernous sinus, orbital apex, pterygopalatine fossa, and various foramina. Thin-section postcontrast axial images acquired by three-dimensional spoiled gradient technique are used in most studies done for intraoperative guidance.
Parasellar lesions
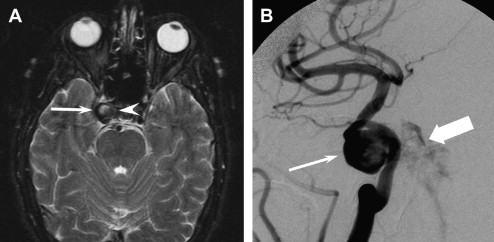
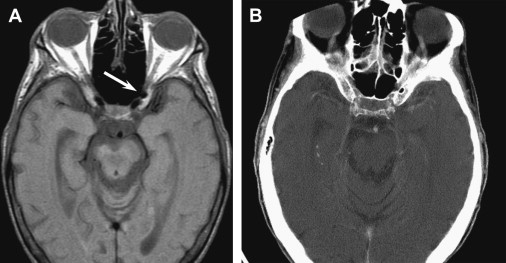
Aneurysms of the cavernous carotid represent a small fraction of all cerebral aneurysms, but figure in the differential diagnosis of cranial nerve palsies. Although catheter angiography remains the gold standard for aneurysm imaging, this diagnosis should always be borne in mind when viewing CT and MRI scans of the skull base. On the most commonly used MRI sequences (spin echo), moving fluid appears as signal dropout (flow void). Unfortunately, any air-containing structure also shows signal dropout. A common and confusing MRI finding is a rounded dark area just anterior to the distal cavernous or proximal supraclinoid internal carotid ( Fig. 4 ). Concern for possible ophthalmic aneurysm often causes a CT angiography (CTA) or MR angiography (MRA) (or even a catheter angiogram) to be performed, but the diagnosis can usually be made using a CT. An intraosseous area of air density can confidently be called normal aeration of the anterior clinoid. CTA and MRA offer noninvasive methods for evaluation of intracranial vessels. Unless bolus timing is very good, CTA of cavernous sinus aneurysms may be suboptimal because early venous filling reduces lesion conspicuity. MRA is preferred for aneurysm detection here, although it is subject to pulsation artifact and to the field distortion that frequently arises from dental amalgam. On noncontrasted head CT examination, an enlarged cavernous sinus often leads to suspicion of aneurysm. This finding is not particularly specific and often arises from ectatic course of the cavernous carotids in older patients.
Rupture of an intracavernous aneurysm does not result in subarachnoid hemorrhage, but may produce a fistula to the cavernous sinus, with resulting increased venous flow here. The actual connection between artery and vein is seldom seen on CTA or MRA examination ( Fig. 5 ). There are usually secondary signs, however, including enlargement of orbital and petrosal veins and superficial cortical veins, exophthalmos, and enlargement of extraocular muscles. Catheter angiography reveals the actual fistulous connection, and whether it is direct (from the carotid artery) or indirect (involving dural vessels).