Lateral Segmental Mandibulectomy
Mark K. Wax
INTRODUCTION
The mandible plays a fundamental role in the form and function of the lower face and upper aerodigestive track. Mastication, speech, deglutition, and protection of the airway are all dependent on a normal, functioning, and intact mandible. Primary tumors of the mandible are rare. The most common malignant tumor to involve the mandible is squamous cell carcinoma arising from the oral cavity or oral pharynx. Rarely the mandible may be affected by cancer of the skin that has grown through soft tissues to invade the mandible or from direct invasion through a metastatic lymph node. These situations are usually related to neglected or previously treated cancer (Fig. 16.1).
When the mandible is involved by cancer, treatment needs to involve resection and usually immediate reconstruction. In processes that involve the mandible primarily, whether they be osteoradionecrosis, primary tumors of dental or alveolar origin, or, rarely, metastatic cancer, a tissue diagnosis must be obtained, which usually involves open biopsy. More commonly, the mandible is involved through direct invasion from a contiguous structure and biopsy of that structure demonstrates the histopathology. The questions then are: (1) Is the mandible involved and (2) can less than a segmental resection of the mandible be performed?
HISTORY
Malignant tumors arising in the oral cavity or oral pharynx that are adjacent to or fixed to the mandible require assessment for mandibular involvement. It is beyond the scope of this chapter to discuss presentation of and the history of tumors rising in the oral cavity or oral pharynx. It is well known that the mandible or periosteum is felt to be resistant to tumor invasion. This resistance disappears in a variety of circumstances. Patients who have had prior radiotherapy, surgical procedures that involve periosteal stripping or resection, or structures close to the periosteum, such as teeth, are more prone to demonstrate invasion of the mandible than those who have not received previous treatment or are distant from the periosteum. Anteriorly, the genioglossus muscle attaches directly into the genioglossal tubercle. Invasion of a primary cancer of the tongue or floor of mouth can track along these muscular processes and invade the mandible (Fig. 16.2). Finally, another route of invasion into the mandible is through invasion of the inferior alveolar nerve/mental nerve. Cancers that have neuropathic tendencies may invade the inferior alveolar nerve through the mental foramen with subsequent invasion of the mandible.
A history of numbness of the lip may indicate that one should look for invasion of the mandible by a neuropathic tumor. If the patient has teeth, then loosening of the teeth or sudden loss of teeth suggests that the patient has invasion of the mandible.
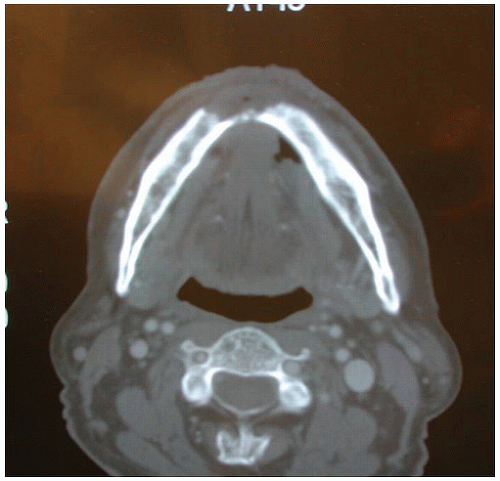 FIGURE 16.1 This patient has let a squamous cell carcinoma of the skin of the chin advance to the stage where it has invaded into the bone of the anterior mandible. |
PHYSICAL EXAMINATION
All lesions of the oral cavity or oral pharynx require thorough inspection and bimanual palpation. Most of the lesions will show separation of the primary tumor from the mandible. When assessing cancers in the retromolar trigone, one oftentimes can see tumor extension over the angle or ramus of the mandible. The tumor may be fixed to the mandible at this location because the mucosa and periosteum are very thin. Examination of the teeth and the alveolar ridge will also help determine if there is an adequate soft tissue margin or if there is, in fact, invasion of the mandible (Table 16.1).
In patients who have been previously treated with radiotherapy or neck dissection and are presenting with a recurrent mass in the neck that is either close to or appears to be fixed to the lateral border of the mandible, an examination with bimanual palpation to demonstrate normal tissue planes or fixation of the mass to the mandible is essential.
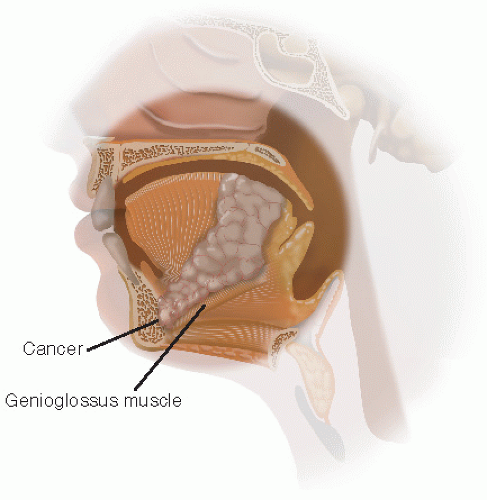 FIGURE 16.2 This artist rendition demonstrates how a cancer can invade along the muscular attachment into the genioglossal tubercle and thus invade the anterior mandible. |
TABLE 16.1 Factors Contributing to Invasion of the Mandible | |||||
|---|---|---|---|---|---|
|
PREOPERATIVE PLANNING
Imaging Studies
Imaging studies are essential in the evaluation and in planning reconstruction for patients who are going to undergo lateral segmental mandibulectomy. Evaluation to assess if there is invasion of the mandible and then the extent of the invasion can be determined by computed tomography (CT) scanning. A fine-cut CT can adequately demonstrate invasion of the mandible and oftentimes the extent of bone involvement (Fig. 16.3). Magnetic resonance imaging can demonstrate limited cortical invasion but often does not define the anatomical structure as well. When invasion of the mandible has been demonstrated on the scan or is highly suspected by physical examination, one needs to determine how one is going to reconstruct the defect. As discussed under surgical technique, most of the time the mandible will be involved on either its superior or medial surface. Consequently, in our experience of over 300 reconstructions using a fibular free flap, a reconstruction plate can be placed at the time of the midline lip split exposure. Occasionally, a lateral segmental mandibulectomy will need to be performed for tumors that have eroded through the mandible. In these cases, it is not possible to prebend a mandibular reconstruction plate before resecting the mandible (Table 16.2). Optimal surgical outcome from a reconstructive, aesthetic, and dental functional perspective is difficult with two free-floating segments of the mandible.
Virtual 3-D Presurgical Planning
Virtual three-dimensional (3-D) presurgical planning is a technology that allows for the generation of custom fitting guides and mandibular reconstruction plates. In this technique, a fine-cut 1-mm 3-D CT is performed. A 3-D construct of the mandible or the maxilla/mandibular complex is then generated on a computer image, which is amenable to 3-D rotation in multiple planes (Fig. 16.4). Once the images are generated, an online
video conference is arranged. The surgeons (ablative and reconstructive), along with a technician who can manipulate the model in three dimensions on the computer screen, plan the ablation and the reconstruction. Determination of the precise locations for where the mandibular osteotomies will be performed and placement of the reconstruction plate is undertaken (Figs. 16.5



video conference is arranged. The surgeons (ablative and reconstructive), along with a technician who can manipulate the model in three dimensions on the computer screen, plan the ablation and the reconstruction. Determination of the precise locations for where the mandibular osteotomies will be performed and placement of the reconstruction plate is undertaken (Figs. 16.5
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
