(1)
Alo Eye Care, Kolkata, India
Keywords
Lateral canthusPeriosteal flapsMyocutaneous flapTenzel’s flap15.1 General Considerations
Tumors involving the lateral canthus are the rarest.
Most lateral canthal repairs are usually performed by using rotational flaps to reconstruct the lateral portion of the upper or lower lid
Since, in principle, the margins must be microscopically tumor-free, the lateral canthal ligament may have to be sacrificed in some cases of lower or upper lid tumour situated laterally.
If only the lateral canthal angle tissue has been excised, a simple advancement flap may be taken from the skin over the lateral orbital wall. The anterior portion is split in two to form the upper and lower limbs and is joined to the upper and lower lid margins. The remnant conjunctiva is mobilized and sutured to the newly formed lateral angle skin with 6/0 continuous absorbable knots. This provides a relatively good cosmetic outcome.

Fig. 15.1
Lateral canthal reconstruction. An ulcerated basal cell carcinoma (BCC) over the lateral canthus

Fig. 15.2
Lateral canthal reconstruction. A circular excision line has been drawn around the BCC. The incision line is extended over the lateral periorbital region, forming the mobilization flap

Fig. 15.3
Lateral canthal reconstruction. A tumor-free margin has been obtained. The incision over the mobilization flap has been deepened and undermined
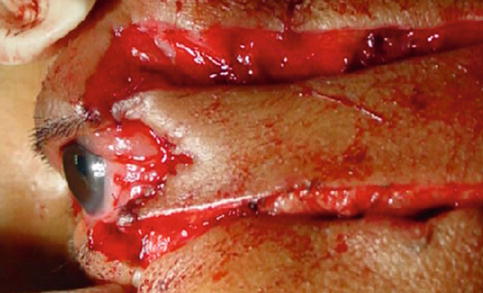
Fig. 15.4
Lateral canthal reconstruction. The anterior part of the mobilization flap has been split to form two limbs from the lateral angle
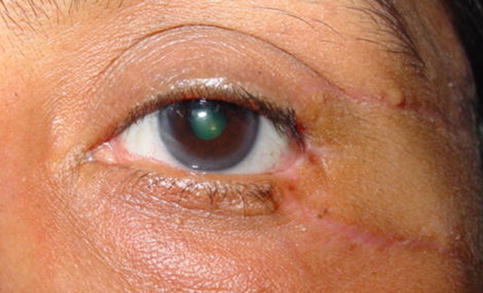
Fig. 15.5
Lateral canthal reconstruction. Six weeks post reconstruction
15.2 Periosteal Flaps
15.2.1 Indications
Lateral canthal area defects in which the upper and lower limbs of the lateral canthal ligament have been sacrificed and only the periosteum over the lateral orbital rim remains.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


