and Charles P. Molumi2
(1)
University of Papua New Guinea and Port Moresby General Hospital, Boroko, National Capital District, Papua New Guinea
(2)
Port Moresby General Hospital, Boroko, National Capital District, Papua New Guinea
2.1 Arytenoidectomy and Lateralization of Vocal Cord (Modified Woodman’s Technique)

Fig. 2.1
A tracheoyomy is usually already performed at the beginning as most of the patients suffer from bilateral abductor palsy
Fig. 2.2
(a) Fiberoptic laryngoscopy shows vocal cords on inspitation and (b) on expiration

Fig. 2.3
A 6–7 cm horizontal incision is given at the level of the lower border of the thyroid cartilage; it extends from the midline to the sternocleiodomasoid muscle laterally

Fig. 2.4
The strap muscles are identified and undermined in a superoinferior direction and retracted laterally
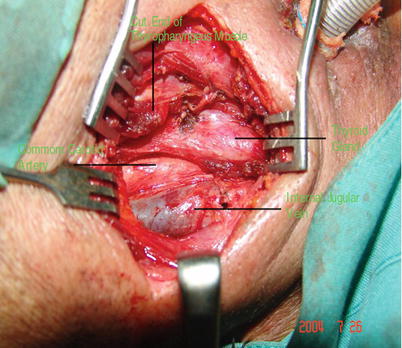
Fig. 2.5
The thyroid cartilage is rotated with the help of a sharp double pronged hook to expose the entire posterior border of the thyroid alar. The inferior constrictor muscle is incised along the entire length of the thyroid alar
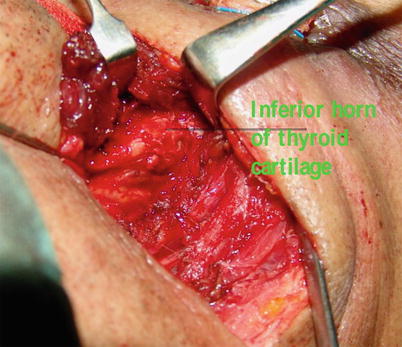
Fig. 2.6
The inferior horn of the thyroid cartilage and the cricothyroid articulation are identified. The cricothyroid joint is disarticulated
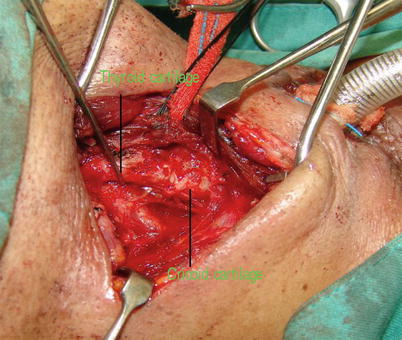
Fig. 2.7
From this step, the operating microscope and the microsurgical instruments facilitate the subsequent steps. The arytenoid cartilage is identified by following the upper border of the cricoid cartilage posteromedially

Fig. 2.8
The muscular attachments are removed and the laryngeal mucosa is reflected from the arytenoid cartilage with finer instruments and microscopic vision. The cricoarytenoid joint is disarticulated and the arytenoid cartilage is carefully retracted laterally to facilitate further separation of the remaining soft tissues from the arytenoid cartilage. The medialward dissection is done carefully to avoid accidental entry into the larynx
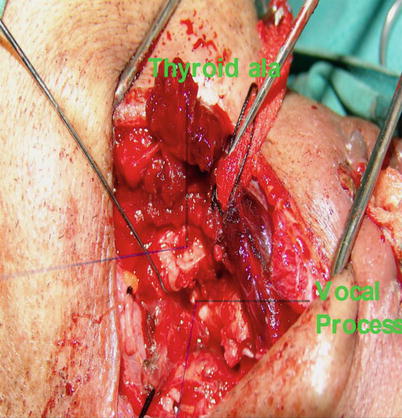
Fig. 2.9
A gentle lateral traction on the arytenoid cartilage exposes the vocal process and the vocal ligament. A 4-0 nylon suture is passed through the substance of the vocal cord around the anterior end of the vocal process. The suture is fixed through a separate holes made at the posteroinferior aspect of the thyroid cartilage. At this stage the thyroid cartilage is returned to the neutral position and the assistant passes a fibreoptic nasolaryngoscope to see the intercordal distance which, after tightening the sutures, should be between 4 and 5 mm. Endoscopic examination also confirm the extramucosal nature of the procedure
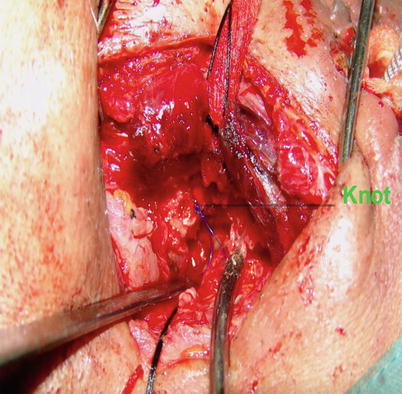
Fig. 2.10
A small knot is placed and the wound is closed in layers after placing a drain
Fig. 2.11
After healing when there adequate airway (a) on expiration and (b) on inspiration during fiberoptic nasolaryngoscopy, the tracheostomy tube is decannulated
2.2 Frontolateral Vertical Partial Laryngectomy

Fig. 2.12
The incision could be a small or a big apron-flap; it depends on the necessity of neck dissection. The tracheostomy could be performed at the beginning or at the end of the procedure
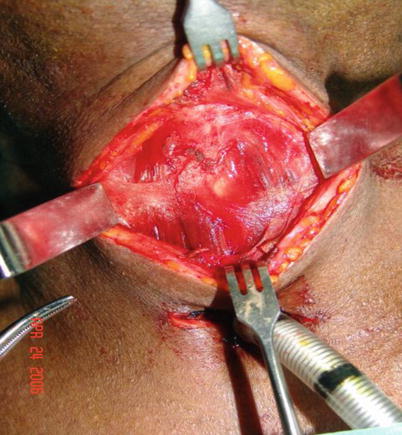
Fig. 2.13
The skin flap is elevated at the subplatysmal level. The strap muscles are separated in the midline. The muscles are retracted laterally using a self-retaining retractor to expose more than the anterior half of the thyroid cartilage
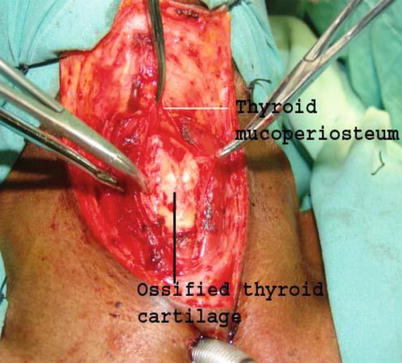
Fig. 2.14
The membrane and the perichondrium attached on the superior and the inferior border of the exposed thyroid cartilage is incised by a scarpal. With the help of a fine elevator, the inner perichondrium of the thyroid cartilage is elevated and the laryngeal soft tissues are separated from each thyroid alar. This step is continued till a paramedian tunnel is created between the upper and lower border of the thyroid cartilage
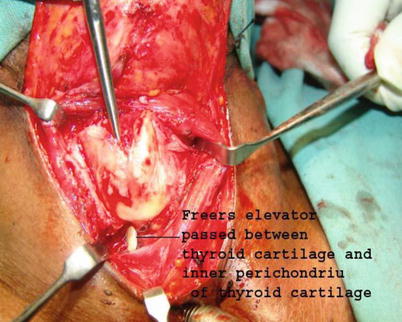
Fig. 2.15
An elevator is placed in the subperichondrial plane for protection of the laryngeal tissue underneath and a triangular portion of the thyroid cartilage is cut; the portion of the cartilage falls equally on either sides of the midline. The triangular portion of the thyroid cartilage is left attached to the underlying laryngeal soft tissues
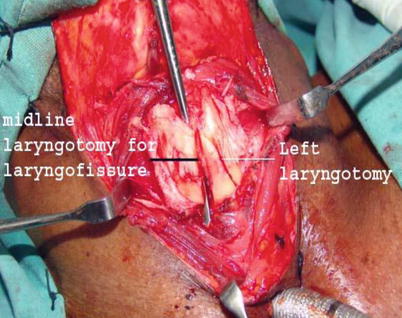
Fig. 2.16
The larynx is entered through the contralateral side (right in this patient) by cutting through the cricothyroid ligament at the inferior border of the thyroid cartilage. The distance of this incision from the midline depends on the extent of the tumor which now could be visualized through the aperture created
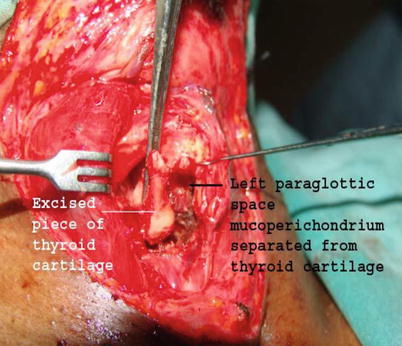
Fig. 2.17
Depending on the extent of the tumor, the inner perichondrium of the involved side is separated in an anteroposterior direction. With the help of a sharp scarple or sickle knife, the superior, the inferior and the posterior margins of the resection are delineated on the left side; it should roughly take the shape of an ‘U’ which opens anteriorly. The degree of posterior resection depended on the tumor extension towards the arytenoid cartilage
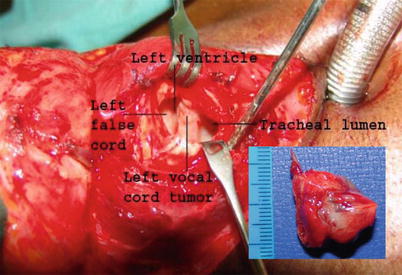
Fig. 2.18
The rest of the attachments of the tumor is cut with a strong curved scissors and the specimen (inset) is removed
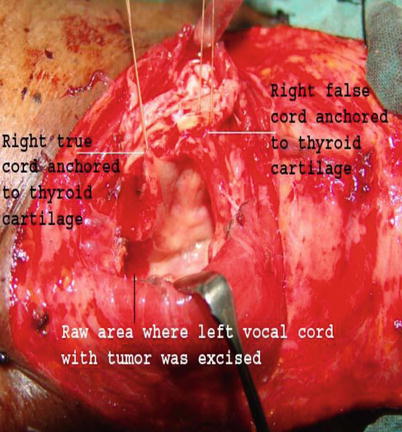
Fig. 2.19
The small raw area is expected to heal by granulation and epithelization
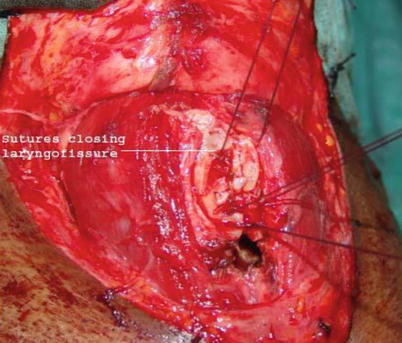
Fig. 2.20
Complete hemostasis is achieved and a tracheotomy is done in case it was not done at the beginning. To prevent the posterior retraction, the true and the false cords of the normal right side are pulled forward and sutured to the anterior border of the ipsilateral thyroid cartilage with fine sutures; these sutures are anchoreed to holes made on the thyroid cartilage with a fine diamond burr as the thyroid cartilage is friable
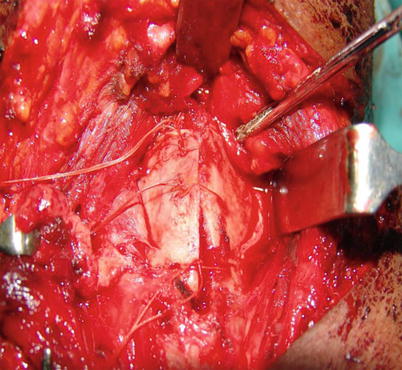
Fig. 2.21
The two halves of the thyroid cartilage are sutured together by a slowly absorbing thick suture material

Fig. 2.22
The strap muscles are reapproxmated and overlapped in the midline in a closed water-tight way over a suction drain. The rest of the incision is closed in two layers

Fig. 2.23
After 4 weeks the raw area is epithelized and the tracheostomy tube is removed
2.3 Supracricoid Laryngectomy with Cricohyoidoepiglottopexy

Fig. 2.24
A ‘U’ type incision is given. It is passed along the anterior border of the sternocleidomastoid muscles, down to the level of the cricoid cartilage. A subplatysmal skin flap is elevated at least 1 cm above the level of the hyoid bone. A functional neck dissection is performed at this stage
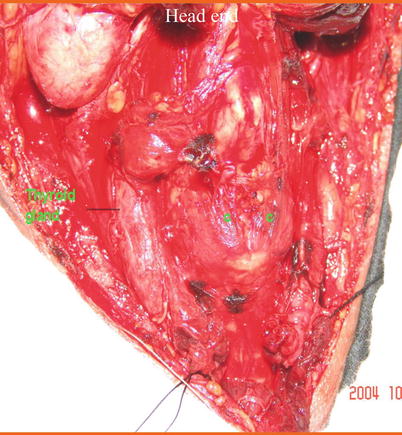
Fig. 2.25
The sternohyoid and thyrohyoid muscles are cut along the upper border of the thyroid cartilage. The former muscles are dissected downwards to expose the sternothyroid muscles. The muscles along the oblique line of the thyroid cartilage (labelled C in the picture) are cut and the larynx is rotated by a hook
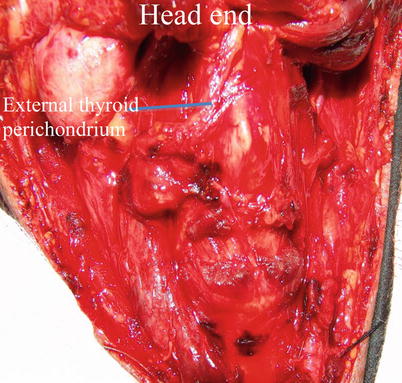
Fig. 2.26
The external thyroid perichondrium and the inferior constrictor muscles are cut along the posterior borders of the thyroid cartilage. Using a perichondrium elevator, the pyriform sinus mucosa is released. The superior laryngeal vessels are identified and ligated, and the internal laryngeal nerves preserved
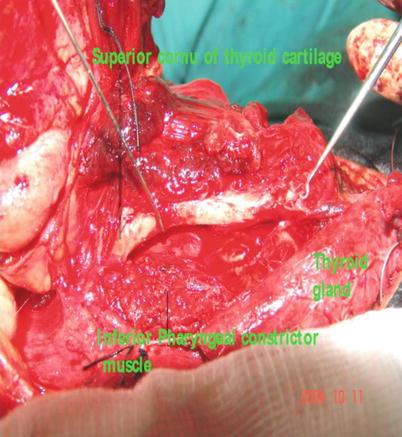
Fig. 2.27
The sternothyroid muscles are dissected downwards beyond the cricoid cartilage thereby exposing the cricothyroid muscles. The muscles are carefully transected to expose the cricothyroid membrane. With the help of the perichondrial elevator, the subglottic mucosa overlying the cricoid cartilage is elevated on the side of the tumor. This step is necessary to achieve wider resection on the diseased side
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


