Laryngoscopy
Laryngoscopy is a key skill that should be mastered by all otolaryngologists. As a diagnostic tool, laryngoscopy can be performed in the office with use of a mirror, rigid telescope, or flexible fiberoptic laryngoscope. Under general anesthesia, rigid laryngoscopes can be used with or without magnification, allowing for accurate diagnosis or manipulation of the larynx when necessary. There are currently a variety of laryngoscopes (both flexible and rigid) available to the otolaryngologist, each with specific features that may aid the surgeon in specific situations. This chapter reviews common techniques for laryngoscopy in the office and operating room setting.
31-1 Mirror Indirect Laryngoscopy
Indications
Mirror indirect laryngoscopy is considered to be part of the basic head and neck examination. It is indicated for patients manifesting with voice complaints or disorders that may manifest with laryngeal pathology. The utility of mirror examination is limited in young children and has largely been replaced by flexible fiberoptic laryngoscopy.
Preoperative Evaluation
No specific evaluations are required for mirror indirect laryngoscopy.
Operative Technique
1. The child is positioned in the upright position seated in a chair or on their caretaker’s lap.
2. The child’s head is extended and the neck flexed in the classic sniffer’s position.
3. The examiner is facing the child using a headlight or head mirror with a focused light source beside the child’s head.
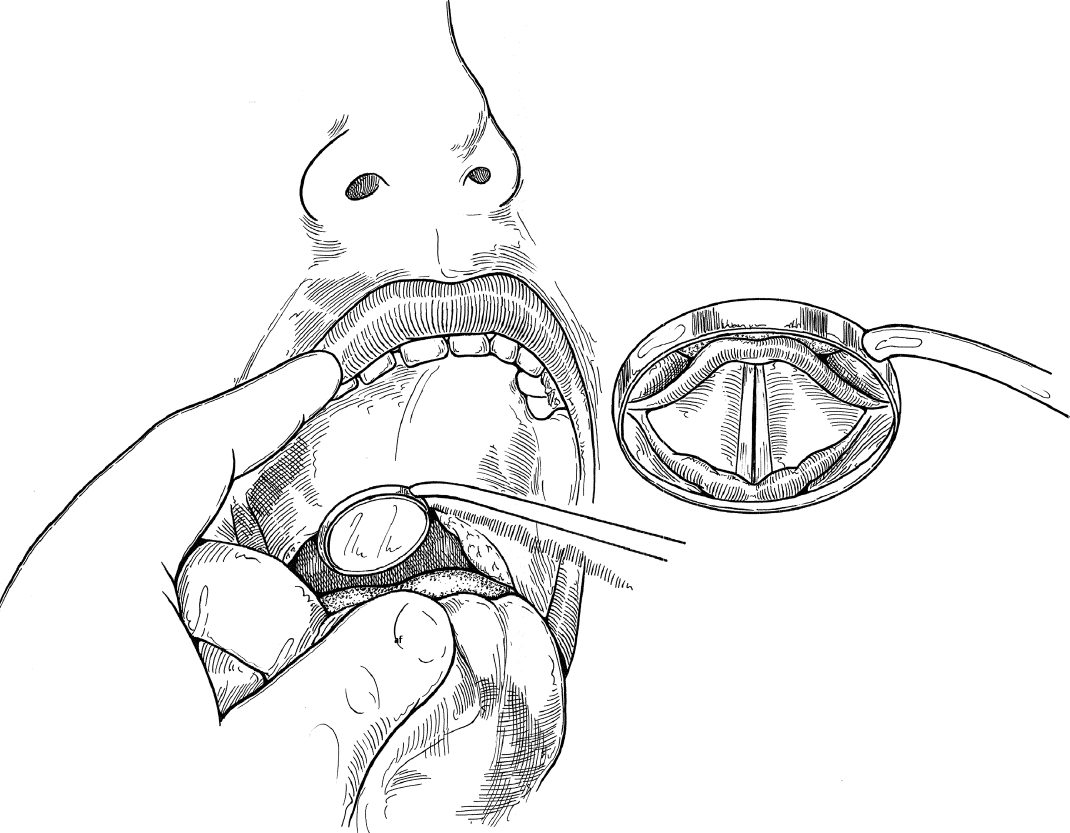
4. The child is asked to open their mouth and protrude their tongue. The anterior portion of the tongue is grasped with a gauze sponge.
5. A warmed or defogged laryngeal mirror is gently inserted into the oral cavity and elevates the uvula and distal soft palate (Fig. 31.1). The warmed mirror should be touched to the examiner’s hand prior to inserting it into the patient’s mouth to prevent burning the oral mucosa.
6. The instrument is angulated until the examiner is able to obtain excellent visualization of the laryngeal and hypopharyngeal structure.
7. The child is asked to say “ee” so that active vocal cord adduction can be observed.
8. If the child begins to gag with the instrument in place, he/she is asked to pant like a puppy. This tends to relax the palate and allows completion of the examination.
Complications
Failure to accurately diagnose pathology
31-2 Rigid Telescopic Indirect Laryngoscopy
Indications
Rigid direct laryngoscopy is a useful technique to accurately assess vocal fold function. It is often used with stroboscopy for patients presenting with voice complaints or disorders that may have visible laryngeal pathology. Compliance with this procedure is limited in young children.
Preoperative Evaluation
No specific evaluations are required for rigid direct laryngoscopy.
Operative Technique
1. This technique utilizes the same preparation as mentioned above.
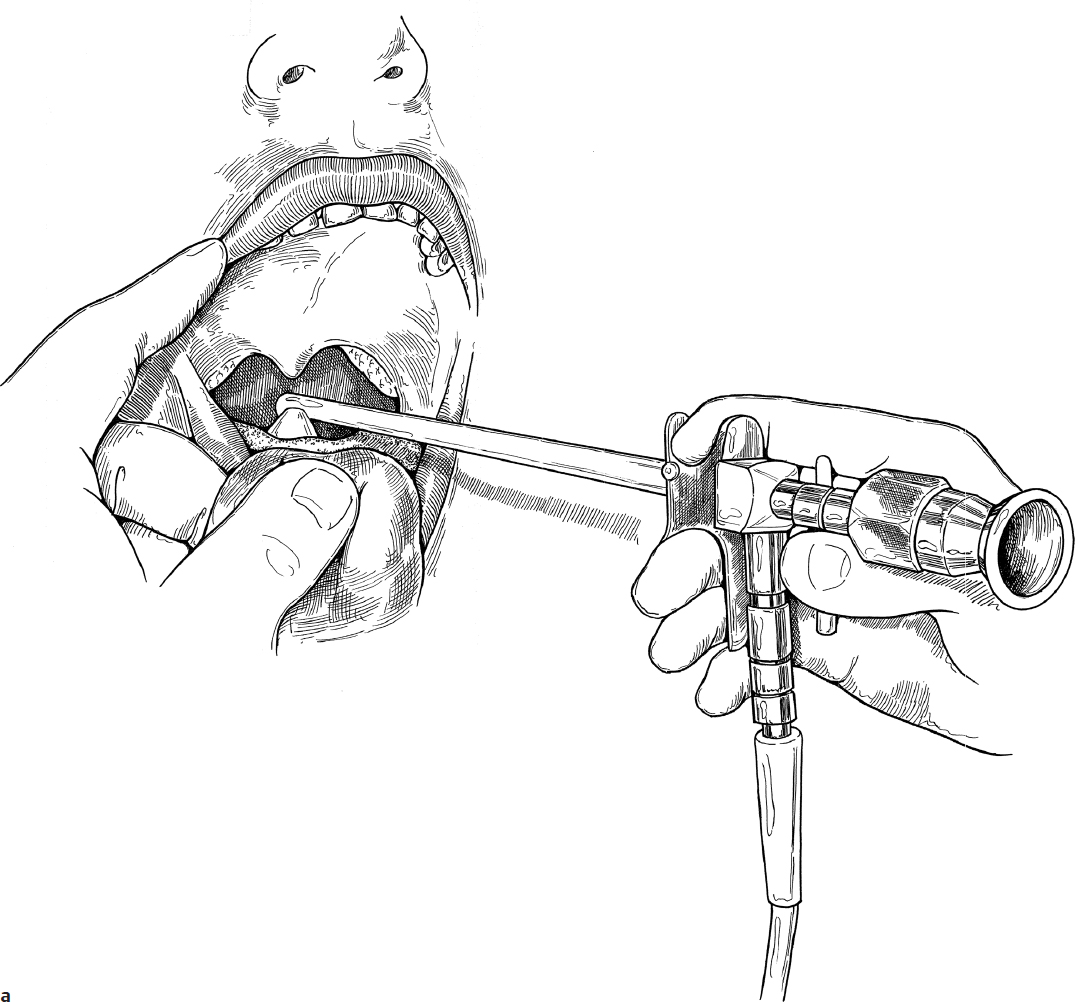
2. The anterior tongue is grasped with a gauze sponge.
3. A defogged telescopic rod with a 90-degree viewing angle is inserted over the surface of the tongue, taking care not to touch the posterior tongue or posterior pharyngeal wall (Fig. 31.2a).
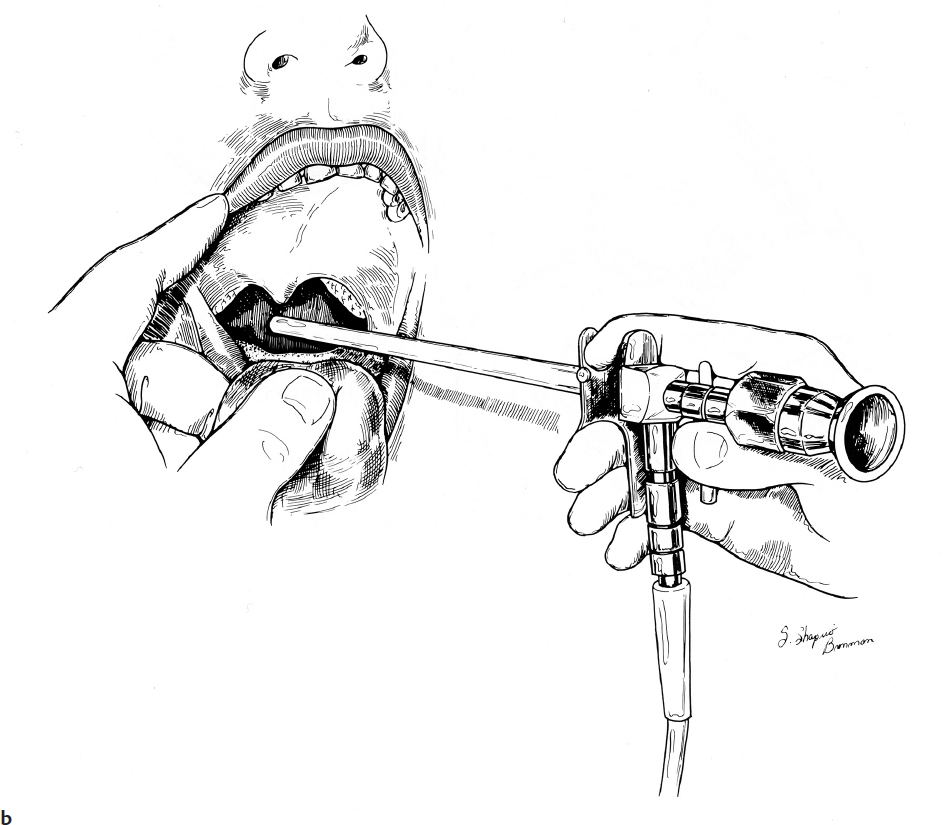
4. Visualization of the laryngeal and hypopharyngeal structures is obtained in the same manner as described for the mirror (Fig. 31.2b).
5. If the child begins to gag with the instrument in place, he/she is asked to pant like a puppy. This tends to relax the palate and allows completion of the examination.
Complications
Failure to accurately diagnose pathology
31-3 Flexible Direct Laryngoscopy
Indications
Flexible direct laryngoscopy is the most commonly used office procedure to assess laryngeal function and pathology in children. Modern flexible laryngoscopes come in sizes as small as 2 mm and allow for excellent visualization of the larynx. The procedure is indicated for patients presenting with voice complaints or disorders that may have visible laryngeal pathology. Additionally, since flexible laryngoscopy does not require alteration of the oral cavity and pharynx by pulling the tongue forward, the procedure can be used to accurately assess the tongue base, hypopharynx, and vocal resonance.
Preoperative Evaluation
No specific evaluations are required for flexible direct laryngoscopy.
Operative Technique
1. The child is seated in the upright position of the caretaker’s lap with the head extended and the neck flexed in the classic sniffer’s position.
2. Flexible direct laryngoscopy may be performed with or without topical anesthesia and/or vasoconstriction. Should topicalization be desired, a 1:1 solution of topical lidocaine (2%) and oxymetazoline may be used.
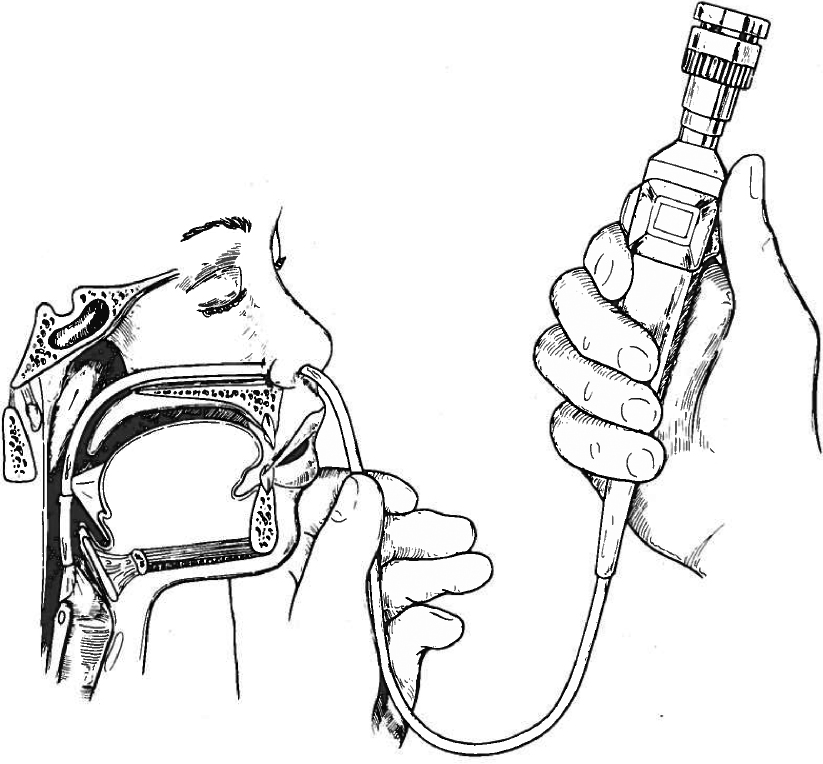
3. The flexible laryngoscope is inserted into the anterior nares and passed posteriorly along the floor of the nose until the nasopharynx is visualized.
4. The scope is flexed inferiorly in the nasopharynx allowing for visualization of the tongue base, hypopharynx, and larynx.
5. The child is asked to say “ee” and laryngeal dynamics are assessed.
6. If aspiration is suspected, the patient may be asked to swallow a variety of food consistencies to assess for laryngeal penetration or pooling (functional endoscopic evaluation of swallowing [FEES]) (Fig. 31.3).
Complications
1. Failure to accurately diagnose pathology
2. Mucosal abrasion
3. Epistaxis